|
Abstract:
Congenital patellar syndrome defined bilateral isolated aplasia
or hyoplasia of patella. This medical condition is different
from Nail-Patella syndrome. This syndrome contain isolated
bilateral aplasia or hyoplasia of patella without any
abnormalitiy. There are few cases about this syndrome in the
medical literature .
We report two cases that have bilateral isolated aplasia of
patella on this paper. And any body abnormalities were not
examined in these two cases. According to databases, this is
very rare medical condition.
J.Orthopaedics 2010;7(4)e6
Keywords:
Case Report:
We report 43 and 14 years-old two cases (both males) had
isolated bilateral aplasia of patella. 43 years old case applied
to our clinic when he was 17 years old and 14 years old case
applied to our clinic befeore one year ago.
Case 1: 43 years-old case applied to clinic
with complaints of deformity in both knees, inability to
straighten the knee, little difficulty in walking and running
and rotationel instability while jogging.
The elder case gave normal birth anamnesis.
In knee measuring of 43 years-old case had 160° flexion and 0°
extanation on both sides. Active and passive movements of the
knees were within normal range, and the quadriceps muscle was of
normal strength with gluteus maximus were good. Nails were
normal. There were no abnomality on his body.
Case 2:
14 years-old case came to our clinic by pediatric consultation
with hardening to walking and going upstairs.
The parents of 14 years-old case gave the history of full term
born, normal delivered child, without deformed knees since
birth. Also there were an anamnesis worsened from the age of 2
years, after he started walking.
In 14 years-old case had more deformity on the right knee,
which made him difficult to walk. Latter case had 35° flexion,
5° extantion loss on right knee and 40° flexion, 0° extantion
loss on left knee. He had an abnormal clinical aspect on his
both knees. And he had not nail-finger anomalies or another
abnomality on his body. The patients immediate family
consisting of his parents and two sisters were examined. To
their knowledge no blood relative had any related knee problem
or any abnormality of their nail sor fingers .The patient was
the last child. The parents were found to have normal patellae
and fingernails.
On physical examination, there were bilateral isolated absence
of patella in both cases. Absence of both patellae and a hollow
sulcus seen in between femoral condyles were the hallmark
clinical features in both cases (figure 1,2,3 and 4). Femoral
condyles were prominent in both cases.

Fig.1

Fig.2

Fig.3

Fig.4

Fig.5

Fig.6

Fig.7
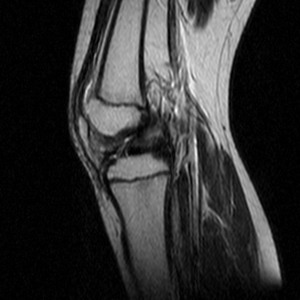
Fig.8
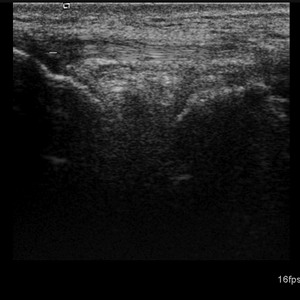
Fig.9

Fig.10
Radiographs and magnetic resonance imaging of both knees showed
absence of both patellae in both cases (figure 5,6,7,8,9,10).
Also ultrasound for case 2 was undergone (figure 11). No other
deformity was present in both patients. No iliac horns were
seen on pelvis x-rays. Examinations of upper limbs and other
systems were clinically and radiologically normal. Blood
parameters were within normal ranges. Genetic studies were
normal. Ultrasounds for abdomen were normal. No renal
abnormalities were noted. Computerized Axial Tomography showed
no the limb length discrepancy and to any other associated
disorders in both lower limbs. Limb lengths were equal on both
sides. No femur or tibial anomalies were seen. Active and
passive resisted physiotherapy had started for both cases. Gait
training was given. The patients were on regular follow up every
3 months in each year. They can do today activities, play,
squat, sit cross-legged and can lead a near normal life.

Fig.11
Discussion :
Congenital absence (aplasia ) of the patella are very rare
anomaly in the human body(1). Congenital patellar aplasia or
hypoplasia associated with genetic disorders belongs to a
clinically diverse and genetically heterogeneous group of lower
limb malformations in the medical literature (2). Also
congenital lower limb malformations without anomalies of the
upper limb are estimated to occur in one of 10,000 live births
(2). These malformations have an autosomal dominant mode of
transmission with 100% penetrance and variable expressivity. And
also this syndrome have been linked on the chromosome with the
ABO blood group gene (2).
The patella is the biggest sesamoid bone of the human skeleton.
And it is formed and located within the tendon of the quadriceps
femoris muscle. Its principal role is to facilitate the extensor
function of the quadriceps muscle and to protect the ventral
cartilage surfaces of the knee joint from other effects (2).
The knee joint is the largest and possibly the most complex
synovial joint in the human body. The patellofemoral joint is a
sellar joint between the patella and the femur. The quadriceps,
anterior cruciate ligament (ACL) and posterior cruciate ligament
(PCL) help to each other for normal arthokinematics of the knee
through the four bar linkage system. Stability of the
patellofemoral joint is proved by the passive and dynamic
factors around the knee. The primary dynamic factor is the
quadriceps muscles. Quadriceps is strong and the extensor
mechanism is enough. This muscle glides in the patellar groove
between the femoral condyles in congenital patella hypoplasia or
aplasia (2).
Isolated absence of patella is extremely rare. Also It usually
causes no disability to the patient. Congenital absence of
patella is only one of several anomalies such as nail patella
syndrome, anomalies of the femur and fibula, dislocation of the
knee, genu recurvatum, clubfoot, or dislocation of the hip,
hypoplastic patella, recurrent lateral dislocation of patella,
genu valgum, slip of medial tibial plateau, cubitus valgus,
hypoplasia of elbow with decreased range of motion, dystrophy in
thumb nails, bifid thumb nails, decrease in the length of
nails, iliac horns, flaring of iliac crests with prominence of
anterior superior iliac spines, pelvic abnormalities. Congenital
absence of patella without any other osseous anomaly is
accompanied by agenesis of the distal third of the quadriceps
muscle or severe lateral dislocation of the extensor mechanism
(2); but in these cases there were no as this condition.
Carbonara ve Alpert notified that Hereditary Osteo-Onycho
Dysplasia (HOOD) showed 92% knee affecting, 11% bilateral
absence of patella. HOOD affects primarily nails, elbows, knees
and pelvis (3). Nail-patella syndrome is a rare genetic
disorder. But it can cause significant morbidity in several
organs, including the musculoskeletal system (4). The
nail-patella syndrome is characterized by abnormalities of the
nails, patella and radial head, iliac crest and, in some cases,
nephropathy. And it showed an autosomal dominant trait. The
genetic defect is localized on chromosome 9q34.1. The clinical
features in affected individuals vary so much. In some cases the
nephropathy may progress to end-stage renal failure, leading to
decreased life expectancy (5); but in these aplastic patellar
cases, we did not find any renal changes in clinical follow up.
Some human developmental syndromes with patellar malformations
may be caused by single gene defects or result in some cases
from mosaic trisomy 8(2).
RAPADİLİNO syndrome, Holt-Oram syndrome,
Meier-Gorlin syndrome,
Genitopatellar syndrome,
Fanconi anemia, Nager syndrome, Coffin Siris syndrome are the
other syndromes that exposed hypoplastic or aplastic patella.
Conclusions:
Congenital patellar syndrome is an extremely rare anomaly. Also
congenital patellar syndrome causes no major disability to the
patient. The treatment is always directed towards the
compliants associated anomalies and matters about the knee (2).
We can say that
the absence of patella show minor importance and requires no
specific treatment. If there are problems as lateral
dislocation, instability, genu recurvatum, discontinuity of the
extensor mechanism, some soft tissue release (lateral
retinaculum release, hamstring release, medial reefing, full
posterior capsule release), proximal and distal alignment
procedures, quadriceps plasty, femoral corrective osteotomy can
be applied (2).
These
soft tissue operations is indicated depending upon individuals
clinical findings. The main goal must be to release soft tissue
contractures and achieve normal alignment for knee functions
(2).
In these two apylastic patellar cases we did not need any soft
or bone tissue operations casuse there are no compliants or
clinical findings. And any renal or other clinical problems did
not develop. Last decision was that congenital syndrome is a
different syndrome from other patellar apylastic/hypoplastic
syndromes.
Reference:
-
Varghese RA,
Joseph
B.,
Congenital aplasia of the patella and the distal third of the
quadriceps mechanism,
J
Pediatr Orthop B.,
2007 Sep;16(5):323-6.
-
J Terrence Jose Jerome, M Varghese, B Sankaran, Congenital
patellar syndrome, Romanian Journal of Morphology and
Embryology 2009, 50(2):291293.
-
Carbonara P, Hereditary Osteo-Onycho Dysplasia (HOOD), Am J
Med. Sci. , 1964, 248: 139-151.
-
Doughty
KS,
Richmond JC.,
Arthroscopic findings in the knee in nail-patella syndrome: a
case report.,
Arthroscopy.
2005 Jan;21(1):e1-5.
-
Wildfeuer T,
Albrecht G.,
Nail-patella syndrome,
Hautarzt.
1996 Nov;47(11):860-2.
|

