| ORIGINAL
ARTICLE |
|
Placement Of Uncemented Acetabular Components In Hip
Arthroplasty Preserving The
Medial Osteophyte [A Prospective Study] |
|
Shyamalan G,
Oppong N
*
Orthopaedic Surgery Unit, Royal Haslar Hospital, Gosport, England.
Address for Correspondence:
Gunaratnam Shyamalan MRCS BSc
Department of Orthopaedics
St. Georges Hospital
Blackshaw Road, London
E-mail: doctorsham@hotmail.com
|
|
Abstract:
An attempt was made to
preserve the medial osteophyte when reaming the acetabulum in 37
patients undergoing total hip arthroplasty over one year. The
patients were examined clinically at six weeks and one year
post-operatively. The medial wall preserved was measured from
the radiographs using a digital system. The mean amount of wall
preserved was 3.16mm and the patients were 100% satisfied with
outcome.Preserving acetabular bone stock, has implications in
acetabular revision surgery.
J.Orthopaedics 2008;5(2)e15
Introduction:
Uncemented hip replacements
are being offered to an increasingly younger population and
revision surgery is inevitable. One of the problems faced by the
revision surgeon is lack of good quality bone stock once the
prosthesis is removed, which then requires other methods such as
bone grafting for coverage. Medial and superior medial cavitary
bone defects are a common problem in revision surgery.1,2,3
Many papers relating to positioning cementless acetabular cups
concentrate on version and inclination. Others on the seating
methods such as line to line reaming with screw fixation or
under-reaming and press-fitting. Advances in uncemented
acetabular cups are generating successful long-term results.4
A common intra-operative
finding in patients with hypertrophic osteoarthritis of the hip
is a large medial osteophyte covering the medial acetabular
wall. However as far as the Author is aware the same principles
of reaming to recreate the head centre, as used in cemented
acetabular replacements are being followed.We propose to show
there is no need to ream down to the medial wall if stability is
not compromised. Preservation of medial osteophyte will preserve
future bone stock and may also remodel in time into a true
medial wall.
Material and Methods :
A prospective study of
thirty seven patients was used. The same surgeon performed the
procedure using his standard default technique, following
manufactures guide lines relating to the cup implantation.5
All patients were operated
on in the lateral decubitus position and a modified Hardinge
approach was used. The acetabulum was exposed and cleared of
fatty tissue and cartilage with a ring curette. The smallest
reamer created the original hemispherical shape and reaming
continued in odd number increments until a tight fit with
reasonable coverage and bleeding underlying bone. A cup, one mm
larger than the last reamer was press-fit in place and as the
cup was rocked the whole pelvis moved as one, indicating a
stable fixation. No attempt was made to medialise the cup
removing the medial osteophyte completely, nor preserving the
medial osteophyte sacrificing implant stability.One or two
screws were fixed to the porous coated shell, followed by the
appropriatepolyethylene liner. A press fit femoral stem was used
in all patients and the neck offset and head size judged by
intra-operative trial reduction and leg length measurements.
Patients were mobilised partial or fully weight bearing. On
clinical review they were asked if they were unsatisfied,
unchanged or satisfied with the outcome.Patients were also
radiographed on day one post operatively and then again at six
weeks and at one year. The radiographs appeared as digital
images on a monitor and these could be calibrated for
magnification. From these images a measurement of the medial
osteophyte could be taken directly from the computer. The six
week films were weight-bearing AP views. The narrowest point
from the implant to the tear drop of the medial wall was
measured and this was taken to be the approximate size of the
medial osteophyte.


Fig. 1 -
Uncemented total hip replacement showing preservation of medial
osteophyte
Results :
We followed up patients
both clinically and radiographically at six weeks and one year.
No complications such as loosening, or continued pain were
observed. There was no adverse effects related to lateralization
of the hip centre such as severe abductor weakness or leg length
inequality at clinical review. There was adequate coverage of
the cup in all 37 patients.
Table 1: Amount of medial wall
preserved as measured from radiographs
|
(mm)of
medial wall preserved |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
Number
of Patients |
4 |
3 |
6 |
11 |
2 |
7 |
2 |
2 |
Mean mm of wall preserved
3.16 mm
Mode mm of wall preserved
3 mm
Median mm of wall preserved
3 mm
There was a 100% patient satisfaction rate
at 6 weeks
Discussion :
In the normal acetabulum,
the bone contour of the femoral head approaches Kohlers
radiographic tear drop to within 5 8 mm. Normal acetabular
forces run roughly from the centre of the hip to the center of
the iliosacral joint, through the subchondral sclerosis zone
sourcil.6
There is evidence to
suggest that a correct head centre, combined with the
appropriate inclination, will prolong the life of the implant.
However this work was done with cemented acetabular implants.7
Measurements varied from 0
7 mm as we first ensured optimal prosthetic positioning to
assure a stable fixation. Each manufacturer has differing
implantation requirements. For example, Depuy Duraloc has a
template for the acetabulum which assumes removal of the medial
osteophyte and starts at the tear drop.8
Most manufacturers can
agree that a good cortical rim fit and a wide area of fixation
to avoid stress concentration is paramount. However studies by
Amstutz 9 have demonstrated that micro-movements
increase when the subchondral plate is removed, herefore
preservation minimizes stress concentration.10
A Swedish group used
radiostereometry to observe the migration of cemented and
uncemented cups. Interestingly the cemented cups migrated
laterally and the uncemented migrated medially, displaying less
radiolucent lines at two years.11 There may be a
remodeling process which occurs creating a new medial wall.
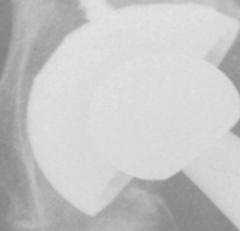
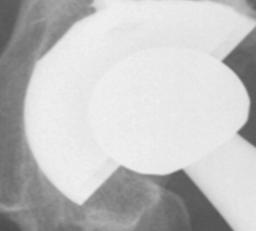
Fig. 2 - Post operative films
showing remodeling at six months.
Preserving the medial
osteophyte without sacrificing implant stability is possible in
uncemented cup arthroplasty. We have now started replacing the
reamings intra-operatively into the medial wall, helping with
medial acetabular coverage in peripherally expanded cups.
Conclusion:
The long term results are
as yet unknown and only time will tell, but the short term
follow-up shows acetabular stability and encouraging signs of
bony remodelling. Preserving bone stock may well have
implications when revision surgery is considered, especially in
cases where failure of the acetabular component has led to
pelvic discontinuity.
Reference :
-
Gross AE. Revision arthroplasty of the acetabulum with
restoration of bone stock. Clinical orthopaedics and related
research 1999Dec (369), P: 198-207.
-
ORourke MR, Paprosky WG, Rosenberg AG. Use of structural
allografts in acetabular revision surgery. Clinical orthopaedics
and related research 2004 Mar (420), P: 113-21.
-
Saleh KJ, Kassim R, Gross AE. Bone assessment and
reconstruction in revision hip surgery. The American Journal of
orthopaedics, 2002 Apr, Vol.3, P: 183-5.
-
Harris WH. Results of uncemented cups: a critical appraisal
at 15 years. Clinical orthopaedics and related research 2003 Dec
(417), P: 121-5.
-
Zimmer. Triology acetabular system. Manufacturers
references.
-
Ochsner PE, Hinchcliffe R. Total hip replacement:
Implantation Techniques and Local Complications. Springer-Verlag
Berlin and Heidelberg GmbH & Co.K, 2002.
-
Hirakawa K, Mitsugo N, Koshino T, Saito T, Hirasawa Y,
Toshikazuk K. Effect of acetabular cup position and orientation
in cemented total hip arthroplasty. Clin Orthop 2001,
388:135-142.
-
DePuy. Duraloc acetabular system. Manufacturers references.
-
Amstutz H. Restoration of functional biomechanics in
reconstructive hip surgery. NIH Consensus Development
Conference, Bethesda, 1982.
-
Jacob H, Huggler A, Dietschi C, Schreiber A. Mechanical
function of subchondral bone as experimentally determined on the
acetabulum of the human pelvis. J.Biomech 9:625, 1976.
-
Digas G, Thanner J, Anderberg C, Karrholm J. Bioactive
cement or ceramic/porous coating vs. conventional cement to
obtain early stability of the acetabular cup. Randomised study
of 96 hips followed with radiostereometry. Journal of
orthopaedic research 2004 Sep, VOL: 22 (5), P : 1035-43.
-
Amstutz HC. Hip Arthroplasty. Churchill-Livingstone, 1991.
-
Canale ST. Campbells Operative Orthopaedics. Mosby, 2002.
|
|
This is a peer reviewed paper Please cite as
:
Shyamalan G : Placement Of Uncemented Acetabular Components
In Hip Arthroplasty Preserving The Medial Osteophyte [A
Prospective Study]
J.Orthopaedics 2008;5(2)e15
URL:
http://www.jortho.org/2008/5/2/e15 |
|
|

