|
*Rajinder Singh Gaheer, +Jamie Mckenzie, ** Maurice Paterson
*
Registrar, Department
of Orthopaedics, Dumfries and Galloway Royal Infirmary, Dumfries,
United Kingdom, DG1 4AP
+
Specialist Registrar,
Department of Orthopaedics, Royal United Hospital Bath NHS Trust,
Bath, United Kingdom, BA1 3NG.
**Consultant,
Department of Orthopaedics, Royal United Hospital Bath NHS Trust,
Bath, United Kingdom, BA1 3NG.
Address for Correspondence
Mr Rajinder Singh Gaheer
10 Maryfield Terrace, Dumfries, United Kingdom, DG1 4UG
Phone: 00(44)1387246246 Ext. 2001
Fax: 00(44)1387241193
Email:
rsgaheer@hotmail.com |
|
Abstract
Sudden onset loss of ankle dorsiflexion is
rarely caused by compression of the common peroneal nerve by
ganglion cysts. Peroneal nerve ganglion cysts typically present
with a palpable mass or features of entrapment neuropathy,
including pain, gradual onset motor and sensory weakness.
Ganglion cysts are common in upper
extremity, most often occurring in the wrist.1 They are
relatively uncommon in the lower extremity, most commonly
involving the peroneal nerve.2 Involvement of the nerve
commonly occurs by compression by these cysts originating from a
neighbouring joint. Compression neuropathy of the peroneal nerve
most commonly presents with pain along its distribution and in
most cases identifiable swelling or mass at the proximal fibula.
For this reason sensory loss or motor weakness is relatively
uncommon. When this occurs, it is gradual and develops over the
course of a period of time because of gradual extrinsic
compression of the nerve. The cases reported here are of two
instances of ganglion cysts arising from the proximal
tibiofibular joint where there was sudden onset of foot drop. No
prior weakness or sensory symptoms were noted and an
identifiable swelling was not reported by the patient. In both
instances lumbar disc disease was thought to be the cause of
footdrop at initial assessment.
Keywords: peroneal nerve, proximal
tibiofibular joint, ganglion cyst, footdrop
J.Orthopaedics 2006;3(4)e20
Introduction:
We report two cases of sudden onset of
footdrop due to ganglion cyst arising from the proximal
tibiofibular joint. Magnetic Resonance Imaging was used to
confirm the diagnosis. Both were successfully treated by
excision of the ganglion cyst.
Case reports
CASE 1
A 67-year-old lady presented to her GP with sudden onset of
right-sided foot drop. She had mild pre-existing back symptoms
but no shooting pain down the leg. There was no history of
trauma. She was referred by her GP to our hospital. On
examination, there was some wasting of the lateral compartment
of the leg. She had reduced sensation over dorsum of foot
distally and less so extending into the front of the shin. There
was Grade 2 power of invertors, evertors, ankle dorsiflexors and
EHL. Plantar flexion was grade 4. Examination of back and hip
was normal. Knee examination was unremarkable as well and
movements were reasonably good with some mild effusion and mild
patello femoral crepitus. Peripheral pulses were intact. Tinel
tap was positive at proximal end of fibula.
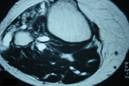
X-ray of the knee was normal. MRI showed a
large well demarcated soft tissue swelling arising from the
proximal tibiofibular joint, (Fig- 1,2). The swelling was
homogenous and had a hypointense signal on T1-weighted images
and hyperintense on T2-weighted images. There was no destruction
of the surrounding bony components. This was causing a visible
compression of the peroneal nerve.
 Surgical
exploration and excision of the cystic
mass was done nearly 9 months after the first symptoms. It was
found to be a large cystic mass communicating with the proximal
tibiofubular joint, (Fig- 3). The nerve was found visibly
scarred at the time of surgery from the pressure of the cyst.
Microscopic examination revealed the mass to be a ganglion cyst. Surgical
exploration and excision of the cystic
mass was done nearly 9 months after the first symptoms. It was
found to be a large cystic mass communicating with the proximal
tibiofubular joint, (Fig- 3). The nerve was found visibly
scarred at the time of surgery from the pressure of the cyst.
Microscopic examination revealed the mass to be a ganglion cyst.
Within two months of the surgery there was
improvement in sensory symptoms. Foot was no longer in inverted
position but was neutral. There was however no active
dorsiflexion yet.
Five months after surgery first flicker of dorsiflexion and
eversion was noticed. There was still some paraesthesia in the
toes. Tinel sign was now in the lower third of the leg.
Nine months later, she was making steady progress. Had grade 3
power of her EHL and EDL and peronei were functioning well at
3+, which were absent previously. She still had some sensory
hypoesthesia in her first cleft. Tinel was now at the ankle.
One year after surgery, there was some altered light sensation
in the foot with very slight weakness of ankle dorsiflexion. She
was able to walk at least one mile without the AFO and cycle two
to three miles without discomfort. Was not on any regular
analgesia and did not use a stick. She did find coming
downstairs difficult but no problems arising from chair.
When last seen in the clinic at two and half years, she was
managing to live her life without too much difficulty though she
cannot walk at speed. She also found that the leg gets a bit
more tired than normal and occasionally aches at night. Repeat
MRI showed osteoarthritis with some early cyst formation in the
knee but no evidence of recurrence in the region of the proximal
tibiofibular joint.
CASE 2
A 48 year old teacher was referred
by her GP for complaints of weakness in the lower left leg with
some paraesthesia in the lateral lower leg, severe left hip/
upper buttock pain and lower back pain.
he first problem to develop was paraesthesia, which he noticed
while playing golf about a year ago. Left groin and buttock pain
developed over the same period. Back pain developed later during
the course of next six months. Pain was aggravated by getting
from sitting to standing, walking, stair use and sudden
movements. He had no morning stiffness. He found driving was
difficult. There were occasional night pains. About three months
ago he suddenly developed weakness in the left lower leg.
On examination he had tenderness at L3- L5 levels with tight
spasm in the left erector spinae. Neurologically there was
complete foot drop and L4-S1 myotomes were weak. There was no
power at all in EDC, evertors or ankle dorsiflexors. His
reflexes were normal but he had numbness in the outer border of
the calf and foot.
MRI showed a small left-sided L5-S1 disc, which was causing some
impression on the S1 nerve root. This however would not explain
the dense weakness that he had in the foot.
On further examination he had a palpable lesion around the
lateral side of the knee, around the proximal end of fibula.
peroneal nerve or running alongside it. The report indicated
that it did not look like a ganglion coming from the knee joint
pushing on the nerve and that it would be remarkably long for it
to be a schwanomma.
Exploration was done and a cystic mass coming from the proximal
tibiofibular joint was identified. This had insinuated its way
into the common peroneal nerve and then intraneurally within the
fascicles about 5 inches upwards within the common peroneal
nerve. Biopsy confirmed that it was an intraneural ganglion.
When last seen in the clinic at a year from surgery he still had
some altered sensation in the distribution of the deep and
superficial peroneal nerves. He had Grade 4 ankle dorsiflexion
and was able to extend all his toes.
Discussion :
Ganglion cysts rarely involve peripheral
nerves. They are easily overlooked as potential causes of
neuropathy during evaluation of clinical cases of nerve palsy.
Ganglion cysts compressing the peroneal nerve can either
originate from the proximal tibiofibular joint causing nerve
dysfunction secondary to compression, they may also arise by
cystic degeneration of the nerve sheath and invade the nerve
appearing as intraneural ganglions. Regardless of their origin,
these have the potential of growing alongside and invading nerve
and thus delay in diagnosis can result in irreversible nerve
damage.2 Many hypothesis have been put forward about the
pathogenesis of these cysts,3 but the hypothesis of synovial
origin from the proximal tibiofibular joint seems most likely.4
This hypothesis enables us to explain the origin of not only
extraneural cysts, but also intraneural ones. In effect, in the
latter case, the cyst lifts and compresses the nerve, and then
produces adherence and fusion between its wall and the nerve
sheath.
The cyst from the proximal tibiofibular joint joins the peroneal
nerve by means of a small recurrent articular branch.15 Spinner
et al 15 stressed the importance of the articular branch and
compared the rate of recurrence before and after the surgeons
awareness of this branch. Prior to identification of this nerve
and failure to address this at operation, there was a higher
rate of recurrence. In both cases described by us, the presence
of connection of the ganglion to superior tibiofibular joint
along the articular branch was identified intraoperatively.
Spinner et al 15 reported six patients in their series of
twenty-four patients who had acute onset of symptoms. Of these,
three patients suffered direct blows to the fibular neck region
(one of which resulted in a fibular neck fracture), two had been
injured during athletic activities and one during a fall. None
of those having sudden onset symptoms however occurred
spontaneously.
The clinical presentation of these can be striking and therein
lies the pitfall of failing to make a timely diagnosis. Swelling
may or may not develop at the lateral aspect of knee, and a
sensory disturbance over the dorsum of the foot may not occur.
Initially only slight weakness in ankle or toe dorsiflexion may
exist, but sudden loss of dorsiflexion may occur as well. In
most reported series, sudden loss of dorsiflexion is a very rare
occurrence. Although ganglion cysts involving the peroneal nerve
typically originate from the proximal tibiofibular joint and
cause nerve dysfunction secondary to compression, they may
alternatively represent cystic degeneration of the nerve sheath
and invade nerve, appearing more as intraneural ganglions.5
Regardless of origin, these mucous filled cysts have the
potential to grow alongside or even invade nerve, and, in that
light, delay in diagnosis can result in irreversible nerve
injury.6
The differential diagnosis involves L5 nerve root pathology, 9
post traumatic intraneural haemorrhage, 10,16 a nerve
compression near the tendinous arch located at the fibular
insertion of the peroneal longus muscle,11 and a nerve sheath
tumour.
Clinical examination may not show any obvious swelling. Plain
radiographs are of little value in the diagnosis of ganglia, but
may be useful in excluding a bony abnormality or fracture of the
neck of fibula. Magnetic resonance imaging is most helpful.
Seegar and Bassett 12 described the characteristics of ganglia
on MRI. On T1-weighted images, the signal intensity is low,
whereas on T2-weighted images, the signal intensity is high and
they appear homogenous. It may be difficult to differentiate a
ganglion from nerve sheath tumours on MRI, as homogeneity of the
lesion is also found in solid masses. The evidence of connection
between the ganglion cyst and the superior tibiofibular joint
capsule or the tail sign, can be best seen in axial slices at
the level of the joint or on sagittal images.15
Ultrasonography may be useful in showing the cystic nature of
the mass and distinguishing it from solid tumours. A combination
of MRI and ultrasonography 7 may be helpful in the differential
diagnosis of doubtful cases.
It is now well known that a permanent cure can be achieved by
microsurgical removal of cyst, respecting the adherent nerve
fibres 13 associated with the ligation or electrocoagulation of
both the pedicle stalk and recurrent articular branch of the
peroneal nerve.14
Obviously when evaluating sudden foot drop, lumbar disc
herniation is the first diagnosis considered and if physical
examination of spine does not point to one anatomic region as
the source of drop, MRI of spine and of the knee may be
necessary. Surgical treatment involves excision of the cyst and
exploration of the peroneal nerve 6,7. There have been reports
of the importance of performing preoperative electromyography
before embarking on exploration. The justification being that if
preoperative electromyography shows tibialis muscle denervation,
complete resolution of palsy is less likely 8.
Conclusion
Treatment of ganglion cyst arising from
the proximal tibiofibular joint must address the underlying
pathoanatomy and should include decompression of the cyst and
ligation of the articular branch of the nerve to avoid
extraneural recurrence. Resection of the superior tibiofibular
joint may also be necessary, but the indications for this
additional procedure are not yet well defined.15 Our cases
illustrates the consideration of proximal tibiofibular cyst as a
cause of sudden foot drop and stress the importance of avoiding
delay in making the diagnosis and performing surgical
exploration and decompression as soon as the diagnosis is
confirmed.
Reference :
-
Sanders WE. The occult dorsal carpal
ganglion. J Hand Surg Br. 1985;10:357-360.
-
Lowenstein J, Towers J, Matthew MT. Am J
Orthop. 2001;30(11):816-819.
-
Brooks DM. Nerve compression by simple
ganglia: a review of thirteen cases. J Bone Joint Surg Br.
1952;34:391-400.
-
Rawal A, Ratnam KR, Yin Q, Sinopidis C,
Frostick S. Compression neuropathy of common peroneal nerve
caused by an extraneural ganglion: a report of two cases.
Microsurgery. 2004;24(1):63-66.
-
Spillane RM, Whitmaan CJ, Chew FS. Peroneal
nerve ganglion cyst. Am J Roentgenol. 1996;166:682.
-
Stack RE, Bianco AJ, MacCarty CS. Compression
neuropathy of the common peroneal nerve by ganglion cysts. J
Bone Joint Surg Am. 1965;47:773-778.
-
Evans JD, Neumann L, Frostick SP. Compression
neuropathy of the common peroneal nerve caused by a ganglion.
Microsurgery. 1994;15:193-195.
-
Parkes A. Intraneural ganglion of the lateral
peroneal nerve. J Bone Joint Surg Br. 1961;43:784-790.
-
Hauax JP, Malghem J, Maldague B, Noel H,
Rombouts JJ, Courtois C, Nagant de Deuxchaisnes C. Pathology of
the upper peroneotibial joint. History of cysts. Apropos of 4
cases. Rev Rhum Mal Osteoartic. 1986;53:723-726.
-
Gurdjian ES, Larsen RD, Lindner DW.
Intraneural cyst of the peroneal and ulnar nerves. Report of two
cases. J Neurosurg. 1965;23;76-78.
-
Sidey JD. Weak ankles. A study of common
peroneal entrapment neuropathy. Br Med J. 1969;3:623-626.
-
Seegar LL, Bassett LW. Tumor and tumour like
conditions. In: Bassett LW, Gold RH, Seegar LL, editors. MRI:
atlas of musculoskeletal system. London: Martin Dunitz; 1989,
p319.
-
Rondepierre P, Martini L, Wannin G, Floquet
J. Intraneural cyst: a rare cause of peroneal palsy. Rev Neurol
(Paris).1990;146:375-376.
-
Fransen P, Thauvoy C, Sindic CJM, Stroobandt
G. Intraneural ganglionic cyst of the common peroneal nerve:
case report and review of literature. Acta Neurol Belg.
1991;91:231-235.
-
Spinner RJ, Atkinson JLD, Scheithauer BW,
Rock MC. Peroneal intraneural ganglia: the importance of
articular branch. Clinical series. J Neurusurg. 2003;99:319-329.
-
Khairallah EW, Weinberg MJ, Maoney J. Acute
common peroneal nerve palsy caused by haemorrhage into a
recurrent ganglion. Can J Plas Surg. 1995;3:209-211.
|

