| CASE
REPORT |
|
Cystic Lesion Of Acromion And Lateral End Of Clavicle In A Case Of
Post Traumatic Acromioclavicular Arthritis
|
|
*Shirish S.Pathak,
Clement Joseph, M.Aravinda, David Rajan
*Department of Orthopaedics,
Sports Injury & Arthroscopy Clinic,
GKNM Hospital, P.N.Palayam ,Coimbatore, Tamilnadu 641037.
India.
Address for Correspondence
Dr.Shirish S.Pathak,
Department of Orthopaedics,
Sports Injury & Arthroscopy Clinic,
GKNM Hospital, Coimbatore, Tamilnadu 641037, India.
Phone:+91-9244401100, +91-0422-2213501
E-mail:drshirishp@yahoo.com |
|
J.Orthopaedics 2006;3(3)e4
Introduction:
The acromioclavicular (AC) joint is a
diarthrodial joint that connects the acromion to the lateral end
of clavicle. Causes for AC joint arthritis are varied including
degenerative osteoarthritis, posttraumatic arthritis, osteolysis
of lateral end of clavicle etc. AC joint post-traumatic
arthritis may develop due to single or repeated episodes of
direct or indirect injury to the joint. Patients complain of
pain in the AC joint area with typical pain on overhead
abduction activities. Special X ray views, CT scan and MRI scan
are useful tools to diagnose this condition .We report a case of
AC joint arthritis with cystic lesions in acromion and lateral
end clavicle which is a rare finding.
Case report:

A 28 years old businessman presented with
pain in right shoulder since 3 years. Patient sustained injury
to right shoulder when doing weight training in gymnasium 3
years back. Pain subsided after 1 month. Patient had
intermittent shoulder pain. He subsequently had a fall from bike
6 months back. After that pain increased in severity and
frequency. Patient also had complaints of pain and difficulty in
overhead abduction activities. Patient had night pain on lying
on same side. There was no history of fever or any instability.
Patient had no other joint pain or systemic illness.
On examination there was tenderness on AC
joint, cross arm test and Obrien test were positive. .
Impingement test & Apprehension test were negative. Terminal
abduction was painfully restricted. AC joint was injected with
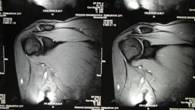
local anesthetic and the pain decreased. X-ray (Zancas view)
showed AC joint arthritis with peculiar finding of cystic
lesions in acromion and lateral end of clavicle. CT scan also
showed cystic lesions in acromion and lateral end of clavicle.
MRI showed increased signal intensity in the AC joint and
subchondral region of lateral end of clavicle and acromion.
Blood investigations were normal. Since the patient did not
respond to previous conservative measures like ultrasound
therapy, surgery was advised.
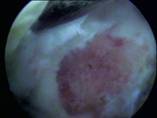
Surgical technique: Patient underwent
arthroscopy in lateral decubitus position through posterior,
anterior and mid-lateral portals. There was no intraarticular
pathology. The lateral end of clavicle was excised using a
motorized burr. The lateral 10 mm of clavicle was excised while
preserving the superior acromioclavicular ligament. The
undersurface of acromion was decorticated to decompress the
cysts (figure-5). At the end of 6 weeks, patient was pain free
with full range of movement. Biopsy report confirmed chronic
inflammatory changes suggestive of posttraumatic arthritis.
Discussion :
Causes for AC joint arthritis are varied
including degenerative osteoarthritis, traumatic arthritis,
post-traumatic osteolysis of lateral end of clavicle4,
atraumatic osteolysis in weight lifters etc.,1,3.
Our patient was young and had two episodes of significant injury
to his right shoulder. Radiological investigations confirmed AC
joint arthritis with a atypical finding of acromion and lateral
end clavicle cysts. Another condition which we thought as a
differential diagnosis was lateral end clavicle osteolysis. The
characteristic findings in osteolysis are osteoclastic
resorption with signs of osteogenesis with widened AC joint and
normal acromion2. In this case these
findings were not present. There was no soft-tissue
calcification which is characteristic of post-traumatic
osteolysis. In literature, there are few reports of cases of
traumatic osteolysis and posttraumatic arthritis with erosive
and cystic radiological changes in the the lateral end of
clavicle. 1,2,4 No report mentions the
presence of cysts in acromion. We report this case of
postraumatic arthritis of AC joint with cyst in acromion and
lateral end of clavicle.
Reference :
-
Scavenius M, Iversen BF. Nontraumatic
clavicular osteolysis in weight lifters.Am J Sports Med. 1992
Jul-Aug;20(4):463-7.
-
Mestan MA, Bassano JM Posttraumatic
osteolysis of the distal clavicle: analysis of 7 cases and a
review of the literature.J Manipulative Physiol Ther. 2001
Jun;24(5):356-61.
-
Shaffer BS Painful conditions of the
acromioclavicular joint.J Am Acad Orthop Surg. 1999
May-Jun;7(3):176-88
-
Zdichavsky M, Hufner T, Pape HC, Rosenthal
H, Tscherne H Unfallchirurg.Post-traumatic osteolysis of the
distal clavicle. A case report and review of the literature
2000 Dec;103(12):1121-3.
-
Zawadsky M, Marra G, Wiater JM, Levine WN,
Pollock RG, Flatow EL, Bigliani Osteolysis of the distal
clavicle: long-term results of arthroscopic resection.
Arthroscopy. 2000 Sep;16(6):600-5
|
|
This is a peer reviewed paper Please cite as
: Shirish S.Pathak: Cystic Lesion Of Acromion And Lateral
End Of Clavicle In A Case Of Post Traumatic Acromioclavicular
Arthritis
J.Orthopaedics
2006;3(3)e4
URL:
http://www.jortho.org/2006/3/3/e4 |
|
|

