|
Abstract:
Neglected rupture of patellar tendon is rare but well recognized
complication of knee trauma. Because they are accompanied by
atrophy and contracture of quadriceps muscle, great deal of scar
formation and poor condition of remaining patellar tendon, these
ruptures are often difficult, technically, to reconstruct a
normal functional extensor mechanism of knee. We report a
74-year-old man with
patellar tendon rupture neglected for 55 years,
treated successfully using Achilles tendon allograft. Sixty
months postoperatively, the active range of motion was 0°~120°
with 5°
of extension lag. Cybex testing showed 70% of quadriceps
strength compared to contralateral limb.
J.Orthopaedics 2010;7(1)e12
Keywords:
Neglected patellar tendon rupture; Achilles tendon allograft
Introduction:
Isolated rupture of the patellar tendon is an infrequent injury
that usually occurs in patients under 40 years of age. Most of
these patients are seen for treatment immediately after injury
and can undergo direct surgical repair with favorable results.1
Surgical management of neglected patellar tendon rupture is more
difficult than that of acute ruptures, and the results are less
favorable because of retraction, adhesion, atrophy of the
quadriceps muscle and proximal patellar migration.1-3
Here, we report a case of patellar tendon rupture neglected for
55 years,
treated successfully using Achilles tendon allograft. Good
functional result was achieved with intensive rehabilitation.
Case Report:
A 74-year-old man visited our department with left lower
extremity weakness with frequent fall. He had a history of blunt
trauma at distal thigh area resulting in a distal femur fracture
with patellar tendon rupture during Korean war at the year of
1950. Bone union was obtained by cast application but management
for patellar tendon injury was not done at that time.
Thereafter, bilateral crutch was used for ambulation because
active knee extension was not possible. Ten years prior to our
visit, extension brace was applied at another institution and
single crutch was used since then. The patients gait was
characterized by forward flinging in swing phase on the affected
leg. The contour and tension of the patellar tendon was absent
in the distal region of patellar. Middle thigh circumference (MTC)
measured at 10 cm proximal to the patellar was 5 cm less
compared to contralateral limb. The passive movement of his left
knee ranged from 0° to 130°; however, there was no active knee
extension. Anterior draw test was positive (grade 3) without
posterior or posterolateral rotatory instability. Radiographs
revealed grade 2 osteoarthritic change according to Kellgren
Lawrens classification4. Distal femur was malunited
with 10° of posterior angulation. High location of patellar was
not visible when compared with the contralateral side. (figure
1) The clinical and radiological diagnosis was confirmed by
magnetic resonance imaging (MRI). T1- and T2-weighted sagittal
images revealed absence of anterior cruciate ligament and
patellar tendon. (figure 2) Fatty degeneration of quadriceps
muscle was not visible.

Figure 1: Lateral preoperative radiograph showing
discontinuity of patellar tendon shadow with malunited distal
femur. Note the position of patellar which is at the same level
compared to contralateral limb.
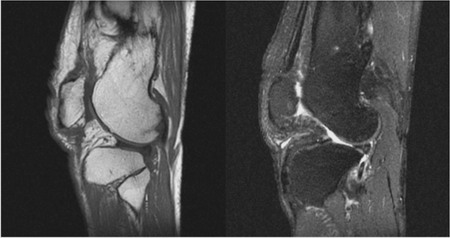
Figure 2: Preoperative MRI of the patients left knee.
Note the discontinuity and wavy pattern of patellar tendon
between patellar inferior pole and tibial tuberosity. Fatty
degeneration of the quadriceps muscle was not visible.
Patellar tendon reconstruction
Reconstruction of patellar tendon was decided to restore active
knee extension and to improve walking ability. A fresh-frozen
Achilles tendon allograft was used. The surgical technique
adopted was similar to that described in Cambells operative
orthopaedics.5 Through an anterior midline approach
and medial parapatellar arthotomy, scar tissue in the remnants
of the patellar tendon was visible with severe adhesion of
fibrous tissue at medial and lateral gutters in suprapatellar
pouch area. (figure 3a,b) For further mobilization, periosteal
elevator was used to dissect the vastus intermedius muscle
proximally off the femur and lateral retinacular release was
performed. The scar tissue at inferior pole of patellar and odd
facet of proximal tibia was excised. After debridement, a
20-mm-long, 20-mm-wide and 15-mm-depth bone trough was created
in the tibial tubercle area slightly distal and medial to the
original insertion of the patellar tendon. This location was
chosen to closely reapproximate the normal direction of pull of
the extensor mechanism, and to simplify closure of the joint
capsule. Contouring the corticocancellous bony portion of the
allograft was done to fit the tibial bony trough and the
tendinous portion was fashioned into three branches, the central
third consisting half the width. This central branch was to be
8~9 mm in diameter. The bony portion was fixed with a single 4.5
mm screw. Kirschner wire was passed through the central part of
the patellar to make a tunnel. 8~9 mm reamer over the Kirschner
wire was passed. Whip stitch with a No. 2 nonabsorbable suture
in the central branch was made and passed through the tunnel
exciting through a slit in the quadriceps tendon. (figure 4)
Multiple interrupted nonabsorbable sutures through the graft in
the soft tissue of the inferior pole of patellar and at the
edges of quadriceps tendon was placed in the position where the
inferior pole of patellar is situated at upper portion of
intercondylar notch at 45° knee flexion. Lateral roentgenogram
was obtained to confirm the patellar height as compared to
contralateral limb. Lateral release closure was done and
patellar tracking was checked. Medial and lateral branches were
tagged to the medial and lateral retinaculum, respectively,
completing the reconstruction.
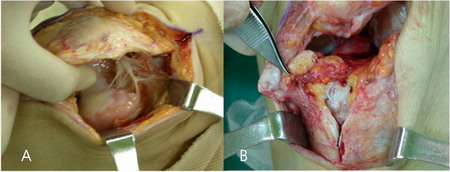
Figure 3.A:Intraoperative photo showing severe soft
tissue adhesion and focal dedudation of femoral articular
cartilage.
Figure 3.B:The degenerative change of free tendinous edge
of the superior portion of the patellar tendon and large gap was
present between the patellar and tibial tubercle.
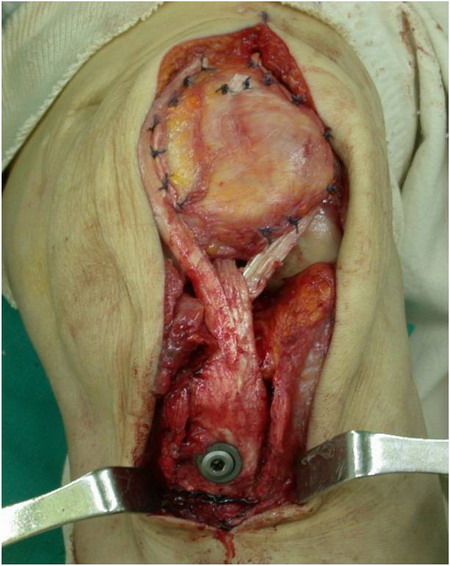
Figure 4: Achilles tendon allograft reinforcing the
retinacular repair from medial and lateral branch. Central
branch is folded through the patellar bone tunnel.
Postoperative rehabilitation
The patient was initially treated in a cylinder cast for two
weeks with the knee in full extension. Continuous passive motion
(CPM) was applied three times daily, beginning at 0°~20° with
close monitoring. The amount of flexion was increased 5°/daily.
At the same time, isometric quadriceps contractions with the leg
in extension were encouraged. He was allowed partial-weight
bearing using Donjoy brace locked at full extension for the
first 4 weeks after the procedure. After 4 weeks after
operation, he started full-weight bearing, had passive ROM of
0°~100°. Three months after the operation, flexion increased to
120°. Finally, 60 months after operation, passive ROM was
0°~120° with 5° of extension lag. (figure 5) Insall-Salvati
index on the operated side was identical to the contralateral
side. Quadriceps muscle strength was estimated by Cybex
examination which consisted of measuring the quadriceps peak
torque at two speeds: 60°/s and 180°/s. Relative strength
reached 70% compared to the contralateral limb. MTC was 2 cm
less compared to contralateral limb. Although he has residual
anterior laxity due to anterior cruciate ligament insufficiency,
he is able to climb stairs respectively without support.

Figure 5: Clinical photo taken 60 months after operation
showing ROM of 0° to 120°. Five degrees of extension lag was
present.
Discussion :
Most patellar tendon ruptures occur as an indirect, low-velocity
injury after minor trauma. Repetitive micro-injuries leading to
tendon weakness usually precede the tendon rupture.
High-velocity injuries are less common and may form a different
entity. The patient recalls to be injured during Korean War at
the year of 1950. He was a soldier then, and blunt trauma to his
left thigh resulted in distal femur fracture. Long leg cast
application was the treatment and bone union was achieved.
Although he was unable to extend his knee after cast removal,
because of personal reasons, he didnt visit any hospital for
nearly 40 years. At initial visit to our department, the patient
had anterior laxity (grade 3) with grade 2 osteoarthritic
change. The initial treatment options were either fusion surgery
or hinged-type total knee arthroplasty. But due to controllable
osteoarthritic symptom and desire of gait improvement with
mobile joint, authors decided to reconstruct the patellar
tendon.
In cases of fresh ruptures of the patellar tendon, which usually
occur at the inferior pole of the patellar, require immediate
surgical restoration of the extensor mechanism for optimal
return to preinjury functional status. End-to-end repair is used
with or without a reinforcing cerclage suture of wire or
nonabsorbable suture material or, alternatively, tape and cast
immobilization is recommended for 68 weeks postoperatively.1
Better results have been reported in immediate repairs of fresh
patellar tendon ruptures in terms of ROM, the strength of the
quadriceps muscle and overall functional results.1
Neglected rupture of the patellar tendon is a rare condition.1,6-8
Simple re-approximation of the torn tendon ends is often
difficult when repair has been delayed more than six weeks
because of quadriceps muscle atrophy and proximal retraction of
the parapatellar soft tissues. Many techniques have been
proposed to address this problem. Fascia lata augmentation with
external fixation using pins and wires was advocated by Siwek et
al.1 Mandelbaum et al3 advised a
Z-lengthening of the quadriceps tendon and Z-shortening of the
patellar tendon with augmentation using the gracilis and
semitendinosus tendons. Levin9 used a Dacron graft to
replace the tendon stumps, immobilized the extremity in a cast
for 6 weeks, and proposed that connective tissue ingrowth would
occur. More recently, Achilles tendon allografts have been used
to replace the patellar tendon, with the bone plug secured into
the tendon insertion at the tibial tubercle, while the
tendionuos part of the allograft is pulled through the tunnels
made in the patellar.10,11
Reconstruction with allograft was decided to our case to avoid
donor site morbidity, as well as earlier restoration of range of
motion and quadriceps strength.
Simple reapproximation of the torn tendon ends is often
difficult when repair has been delayed more than 6 weeks.1
The longer the delay between injury and repair, the greater the
likelihood of quadriceps contraction and proximal patellar
migration. Patients with a neglected rupture of several months
duration may require preoperative patellar traction.1
This can be accomplished over the course of several days to
weeks with the use of a 5-lb weight pulled distally through a
Steinmann pin placed transversely through the midportion of the
patellar. An external fixation device consisting of two
transverse Steinmann pins (one through the patella and one
through the tibia) connected by a Charnley compression clamp may
be used for reducing tension across the repair or
reconstruction.2 Most of these cases, some form of
quadricepsplasty are needed. Our case, although 55 years after
trauma, did not show much proximal migration. When patellar
tendon rupture occurs, it is known that the fibrous adhesions
develop between the patellar and the underlying femur. Long leg
cast application to treat distal femur fracture at the time of
injury may have had a preventive role of proximal migration of
patellar. Operative findings showed severe adhesions and
fibrotic band formation from patellar to the medial and lateral
gutters in suprapatellar pouch area and between vastus
intermedius muscle to the femur. Meticulous release was needed
to mobilize patellar. Although adhesions were severe, quadriceps
muscle contractures were not definite, making quadricepsplasty
unnecessary. In preoperative MRI, fatty degeneration of
quadriceps muscle was not prominent. All of these factors, in
our experience, may have contributed to successful functional
result.
In our case, reconstruction of a 55-year-old neglected patellar
tendon rupture with Achilles tendon allograft gave an reasonable
functional result. Patellar alignment and active range of motion
of the left knee were much restored and maintained.
Reference :
-
Siwek CW, Rao JP. Ruptures of the extensor mechanism of the
knee joint. J Bone Joint Surg Am. 1981; 63:932-937.
-
Takebe K, Hirohata K. Old rupture of the patellar tendon. A
case report. Clin Orthop Relat Res. 1985:253-255.
-
Mandelbaum BR, Bartolozzi A, Carney B. A systematic approach
to reconstruction of neglected tears of the patellar tendon. A
case report. Clin Orthop Relat Res. 1988:268-271.
-
Kellgren JH, Lawrence JS. Radiological assessment of
osteo-arthrosis. Ann Rheum Dis. 1957; 16:494-502.
-
Azar FM. Traumatic disorder. In: Terrry CS, ed. Campbell's
Operative Orthopaedics. vol 3. 10th ed. Philadelphia:
Mosby; 1998:2470-2472.
-
Kelikian H, Riashi E, Gleason J. Restoration of quadriceps
function in neglected tear of the patellar tendon. Surg
Gynecol Obstet. 1957; 104:200-204.
-
Ecker ML, Lotke PA, Glazer RM. Late reconstruction of the
patellar tendon. J Bone Joint Surg Am. 1979;
61:884-886.
-
Shepard GJ, Christodoulou L, Hegab AI. Neglected rupture of
the patellar tendon. Arch Orthop Trauma Surg. 1999;
119:241-242.
-
Levin PD. Reconstruction of the patellar tendon using a dacron
graft: a case report. Clin Orthop Relat Res.
1976:70-72.
-
Falconiero RP, Pallis MP. Chronic rupture of a patellar
tendon: a technique for reconstruction with Achilles
allograft. Arthroscopy. 1996; 12:623-626.
-
McNally PD, Marcelli EA. Achilles allograft reconstruction of
a chronic patellar tendon rupture. Arthroscopy. 1998;
14:340-344.
|

