|
*C McLean,
J Oakshott, P Patel, R
Heywood, M Darbyshire and J Pike
*Department of Trauma & Orthopaedics,
Frimley Park MDHU, Frimley, Surrey, UK
Address for Correspondence
Department of Trauma & Orthopaedics, Frimley Park MDHU, Frimley,
Surrey, UK
Email:
christopher.mclean@fph-tr.nhs.uk
|
|
J.Orthopaedics 2005;2(3)e4
Case report
A
thirteen year old adolescent presented to our accident and
emergency department with a closed, displaced fracture of his
metaphyseal distal tibia and fibula. He had fallen from a
height of approximately two metres. He had been
 attempting
to jump over a gap between two walls onto attempting
to jump over a gap between two walls onto a ledge on an urban building. Following a sprint run-up he
cleared the gap but overshot the ledge and fell onto his
extended left leg in heel strike. He was taken to hospital and
referred to the on call orthopaedic surgeons approximately two
hours after his injury with a deformed left leg. At that stage
he had diminished sensation to light touch on the dorsum of his
foot and his dorsalis pedis pulse was weaker compared with the
right side. His fracture was reduced emergently in the accident
and emergency department under sedation in order to alleviate
his neurovascular compromise and he was placed into a split
above knee plaster of Paris cast. His neurovascular compromise
was relieved immediately and he remained well overnight. A
formal manipulation under anaesthesia was performed the next
day, when he was appropriately starved and a satisfactory
reduction was achieved. The reduction was not anatomic as the
extent of the impaction of the anterior aspect of the distal
fragment was such that fracture was unstable
a ledge on an urban building. Following a sprint run-up he
cleared the gap but overshot the ledge and fell onto his
extended left leg in heel strike. He was taken to hospital and
referred to the on call orthopaedic surgeons approximately two
hours after his injury with a deformed left leg. At that stage
he had diminished sensation to light touch on the dorsum of his
foot and his dorsalis pedis pulse was weaker compared with the
right side. His fracture was reduced emergently in the accident
and emergency department under sedation in order to alleviate
his neurovascular compromise and he was placed into a split
above knee plaster of Paris cast. His neurovascular compromise
was relieved immediately and he remained well overnight. A
formal manipulation under anaesthesia was performed the next
day, when he was appropriately starved and a satisfactory
reduction was achieved. The reduction was not anatomic as the
extent of the impaction of the anterior aspect of the distal
fragment was such that fracture was unstable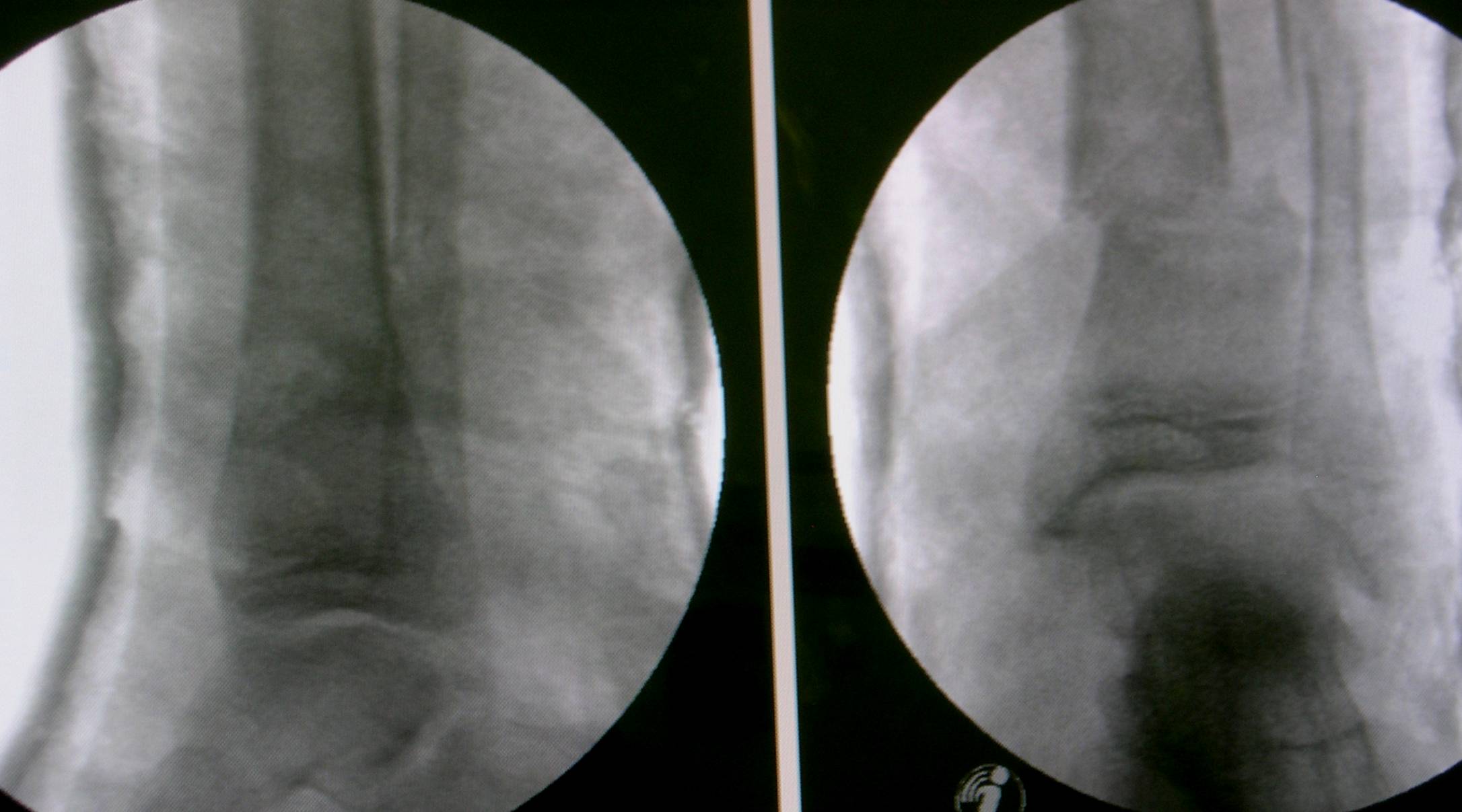 readily angulating into both varus or valgus. The best
stability was achieved with the distal fragment translated
approximately twenty percent laterally, in this configuration
the fracture remained anatomically reduced on the lateral film
and there was no angular or rotational deformity. An above knee
plaster of Paris cast was applied with the ankle fully
plantar-flexed in order to control the recurvatum deformity. He
was discharged two days later for follow-up in his local
fracture clinic.
readily angulating into both varus or valgus. The best
stability was achieved with the distal fragment translated
approximately twenty percent laterally, in this configuration
the fracture remained anatomically reduced on the lateral film
and there was no angular or rotational deformity. An above knee
plaster of Paris cast was applied with the ankle fully
plantar-flexed in order to control the recurvatum deformity. He
was discharged two days later for follow-up in his local
fracture clinic.
Discussion
Fractures of the metaphyseal distal tibia and fibula are not
common fractures in children being only the third most common
long bone to fracture. According to Rockwood ankle fractures,
including the metaphyseal distal tibia, account for 4.4% of all
paediatric fractures. These fractures are often greenstick. In
contrast our patients fracture was one hundred percent
displaced as a result of the comparatively violent mechanism of
injury he sustained. The violence of his injury accounted for
his initial deformity, subsequent impaction of the anterior
aspect of his distal fragment and consequential non-anatomic
reduction. Nevertheless adequate stability was achieved without
the need for percutaneous pins. Our patients skeleton is close
to maturity and in keeping with his adolescent status his
fracture had a combination of adult and paediatric features. He
was a high school student participating in an unorganised
physical activity this combination is associated with a high
incidence of sport related injury [5]. His fracture occurred in
the lower limb as opposed to the upper limb. Upper limb
injuries are more typical for children as they have a tendency
to fall head first and land on their upper limbs or skulls
[2,3]. The injury risk factor for Parkour is unknown Chambers
defined this concept in a study of six American sports in 1979.
He studied the risk factors that contributed to fractures and
dislocations during athletic events. The injury risk factor was
a function of the number of injuries, number of participants,
duration of the participation and the duration of the sporting
season [1]. Our patient had been attempting to perform an
acrobatic leap as part of a Parkour activity. Parkour may also
be known, as the art of movement, free-running, or obstacle
coursing is an activity invented in the Paris suburbs by David
Belle and Sebastien Foucan. Parkour consists of finding new and
potentially dangerous ways to traverse the city landscape. The
activity is a way of using obstacles in ones path in order to
perform jumps and acrobatics. It involves the scaling of walls,
roof-running and leaping from building to building. In essence
it can be thought of as an extreme sport that combines aspects
of free hand rock climbing with gymnastics in an urban setting.
Enthusiasts of the activity may refer to themselves as
Parkouristes or traceurs. Some Parkour enthusiasts claim that
the activity is not just a recreation rather it is a form of art
or even akin to an eastern philosophy requiring discipline,
self-improvement and interdependence. Parkour beginners are
encouraged to start with the basic manoeuvres, in groups,
avoiding high walls and with the use of protective equipment.
Information regarding Parkour is readily available on the
internet, a search using the google search-engine revealed over
73,000 matches. Our patient was new to Parkour, having gained
his first exposure to it two days before his injury in a
television documentary he had watched. As such he was
performing a difficult jump, on an unfamiliar obstacle he was
on a visit to our hospitals locality without the use of any
protective equipment and without any previous Parkour training.
The phenomenon of children participating in dangerous television
inspired activity is well known. Children who watch television
depicting physical risk taking are more likely to take physical
risks themselves [4]. Whilst there are no other reports of
injuries sustained during Parkour mentioned in the medical
literature, it is surely only a question of time before a
substantial number of case series are described. Consequently
traumatologists should familiarise themselves with Parkour and
its risks and advise those wishing to participate in the
activity of the inherent dangers associated with the recreation
and means by which these may be reduced.
REFERENCES
1) Chambers R. Orthopaedic
Injuries in Athletes Ages 6 to 17: Comparison of Injuries
Occurring in Six Sports. American Journal Sports Medicine 7:
195, 1979.
2) Hanlon C, and Estes W. Fractures in ChildhoodA Statistical
Analysis. American Journal of Surgery 87: 312, 1954.
3) Iqbal Q. Long-Bone Fractures Among Children in Malaysia.
International Surgery 59: 410, 1975.
4) Potts R, Doppler M, Hernandez M. Effects of television on
physical risk taking in children. Journal of Experimental Child
Psychology 58: 321-331, 1994
5) Zaricznyj B, Shattuck L, Mast T, Robertson R,
and D'Elia G. Sports-Related Injuries in School-Aged Children.
American Journal Sports Medicine 8: 318, 1980.
|

