|
Abstract:
Open reduction and internal fixation
(ORIF) of fractures with implants and prosthesis has become the
predominant modality of treatment of fractures in most trauma
centers. Incidentally, this is associated with postoperative
wound infection (POWI) reported to be in the range 0.8 to13%.
The aim of the study was to study the occurrence and sensitivity
pattern of various infections in orthopaedic patients for a
better management, thereby reducing both mortality and costs.
Multidrug resistant gram negative isolates causing SSIs and UTIs
predominated in orthopaedic patients. Moreover the rate of
infection was relatively high in patients of open and multiple
fractures .
J.Orthopaedics 2010;7(2)e3
Keywords:
SSIs;Nosocomial infections;Antimicrobial resistance
Introduction:
Nosocomial infections are a
significant problem throughout the world and rates range from as
low as 1% in a few countries in Europe and America to more than
40% in parts of Asia, Latin America and Sub Saharan Africa.1
However during the past few years , there has been a
remarkable improvement in the field of diagnosis of orthopaedic
infections due to newer techniques and sophisticated tools,
better health care systems , particularly in urban areas ,
increasing awareness of patients and invention of newer more
effective and less toxic antimicrobials for combating
osteoarticular infections.2 Open reduction and
internal fixation (ORIF) of fractures with implants and
prosthesis has become the predominant modality of treatment of
fractures in most trauma centers.3 This is not only
because of the better understanding of biomechanics of
implantable materials but more importantly because of the better
functional outcome in these patients.3,4 ORIF is a
major procedure to alleviate pain and to improve mobility in
people with damaged joints. Less than 10% of
prosthesis recipients develop implant associated complication
during their lifetime, predominantly as aseptic failure.
Incidentally this is associated with postoperative wound
infection (POWI) reported to be in the range 0.8 to13% , for
both deep and superficial infections with attendant morbidity
and cost. 5 The microbiology of POWI and their
relative rates vary from one hospital to another . In Nigeria,
Mbamali6 observed that in 60% of his patients with
implant infection ,the etiological agent was S.aureus.
Other organisms isolated in that study were Pseudomonas
pyocyanea and Klebsiella spp. Oguachuba7
found that in 41.9% of the wounds, infections were caused by
Proteus spp. while S.aureus accounted for 25.6% of
cases. Coliforms (13.9%), Streptococcus spp.,
Pseudomonas spp. and Klebsiella spp.were
the other isolates reported by this author. However the pattern
of isolates from USA was slightly different in which gram
negative organisms predominated 8.
Limited studies are available in
Indian literature regarding prevalence of nosocomial infections
in orthopaedic patients, their etiological agents and
antimicrobial sensitivity pattern of isolates. So the present
study was conducted to delineate the occurrence and sensitivity
pattern of such infections for a better management, thereby
reducing both mortality and costs.
Materials
and Methods:
Study centre :
This was a prospective study carried out at a tertiary care
hospital in India over aperiod of one year.
Patient selection:
One hundred and ninety eight patients, who were admitted in the
orthopaedic ward were included in the study. Various samples
like throat swabs, nasal swabs, urine and swabs from surgical
sites were collected aseptically from all patients admitted for
surgery at the time of admission. Patients with any evidence of
infection at the time of admission were excluded from the study.
Similar samples were collected after 48 hours of hospital stay
from the same patients.
Processing of specimens:
Swabs from open fractures , bed sores and wounds clinically
suspected to be infected were collected with all aseptic
precautions to avoid contamination and were immediately
transported to the Microbiology laboratory. The pathogens were
identified by standard laboratory procedures including grams
staining ,motility ,colony characters and biochemical
reactions. 9Antibiotic susceptibility testing was
done by Kirby-Bauer disc diffusion method .10
Following antimicrobials were used
(A)
For Gram positive aerobic isolates:
Penicillin (2 units), oxacillin (1mg),
cephalexin (30mg)
doxycycline(30mg),erythromycin
(15mg),
clindamycin (2mg),
linezolid(30mg),
cotrimoxazole (25mg),vancomycin
(30mg),
ofloxacin (5mg),
gatifloxacin (5mg),
amoxycillin / clavulanic acid (20mg/10mg
), pristinamycin (15mg
) .
(B)
For Gram negative aerobic isolates:
Amoxycillin (10mg),
cephalexin (30mg),
gentamicin (10mg),
amikacin (30mg),
amoxycillin / clavulanic acid (20mg/10ug),
piperacillin/tazobactam (100mg/10mg),
cefepime (30mg),
ceftazidime/clavulanic acid (30mg/10mg),cefoperazone/sulbactam
(75mg/30mg),
cefotaxime (30mg),
ciprofloxiacin (5mg),meropenem
(10mg),
aztreonam (30mg),
ceftazidime (30mg),
netilmicin (30mg),
gatifloxacin (5mg)
.
(C)
For Pseudomonas species:
Ceftazidime (30mg),
gentamicin (10mg),
amikacin (30mg),
piperacillin/tazobactam (100mg/10mg),
cefepime (30mg),
cefoperazone/sulbactam (75mg/30mg),
aztreonam (30mg),
ofloxacin (5mg),
imipenem (10mg),
, ceftriaxone (30mg)
, netilmicin(30mg),
ceftizoxime (30mg).
All the antibiotic discs used were obtained from Hi-Media
Laboratories Pvt. Ltd.
Results :
Study population and patient characterstics:
From the total number of 198
patients investigated in the present study , 76.3% were males
and 23.7% were females and their ages ranged between 5 to 83
years with a mean age of 42.06 years.
Incidence of various types of infection :
Based on the results of culture
,37(18.6%) had a positive bacterial culture. Among three
patients of UTI, Candida albicans was isolated. The
incidence of various types of infections in 198 patients
enrolled for the present study in relation to orthopaedic
illness and procedures is described in the table 1.
Table 1: Site wise
distribution of bacterial isolates in relation to orthopaedic
illnesses and procedures
|
Clinical diagnosis
|
|
No. of isolates |
Site |
|
Number |
Surgical |
Urine |
Throat |
Nose |
|
Fractures |
89 |
14 |
9 |
4 |
1 |
- |
|
Multiple fractures
with road side accidents |
42 |
10 |
8 |
2 |
- |
- |
|
Spinal injury |
12 |
4 |
1 |
2 |
1 |
- |
|
Tendon and ligament
injuries |
6 |
0 |
0 |
0 |
0 |
0 |
|
Amputation |
5 |
2 |
2 |
- |
- |
- |
|
Cellulitis |
5 |
1 |
- |
- |
1 |
- |
|
Osteomyelitis
|
5 |
1 |
1 |
- |
- |
- |
|
Abscess |
4 |
1 |
- |
- |
- |
1 |
|
Spina bifida
|
1 |
0 |
- |
- |
- |
- |
|
Miscellaneous |
29 |
4 |
1 |
2 |
1 |
0 |
|
Total |
198 |
37 |
22 |
10 |
4 |
1 |
Pathogens :
Most frequently isolated organisms
were S.aureus ( 22.5%) ,E. coli (20%), K.
pneumoniae (17.5%), Enterobacter spp(10%), P.
aeruginosa (10%), Citrobacter spp. (7.5%) and A.
baumanii (5%) and Candida albicans (7.5%). SSIs and
UTIs were observed in 18.6% and 11.1% of patients respectively (
Table2).
Table
2: Distribution of various bacteria isolated in various
nosocomial infections
|
Gram positive bacteria |
SSIs |
UTIs |
Nasopharynx |
|
(n) |
(%) |
(n) |
(%) |
(n) |
(%) |
|
S. aureus |
7 |
31.8 |
2 |
20 |
- |
- |
|
E. coli |
6 |
27.3 |
2 |
20 |
- |
- |
|
K.pneumoniae |
4 |
18.3 |
1 |
10 |
2 |
40 |
|
Enterobacter spp. |
1 |
4.5 |
1 |
10 |
2 |
40 |
|
P.aeruginosa |
3 |
13.6 |
1 |
10 |
- |
- |
|
Citrobacter spp |
- |
- |
3 |
30 |
- |
- |
|
A.
baumanii |
1 |
4.5 |
- |
- |
1 |
20 |
|
|
22 |
100 |
10 |
100 |
5 |
100 |
Antimicrobial susceptibility pattern:
Table 3 shows the antibiotic
sensitivity pattern of various gram negative isolates other than
P.aeruginosa from orthopaedic patients.
Table 3:
Resistance pattern of gram-negative bacteria other than
P.aeruginosa from orthopaedic patients
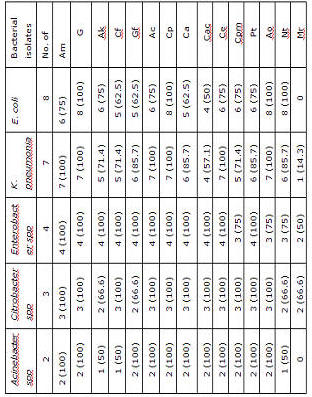
Am : amoxycillin, G : gentamicin, Ak : amikacin, Cf
:ciprofloxacin, Gf : gatifloxacin , Ac : amoxycillin/clavulanic
acid, Cp : cephalexin, Ca : ceftazidime, Cac : ceftazidimne/clavulanic
acid, Ce : Cefotaxime, Cpm : cefipime Pt : Piperacillin/tazobactam,
Ao : aztreonam, Nt : netilmicin, Mr : meropenem.
Figures
in parenthesis indicate percentages.
Among the 9 isolates of S.aureus
,four were MRSA. Resistance to other tested drugs ranged
from 33% to 77%. However, no isolate showed resistance to
vancomycin and linzeolid. All the strains of P.aeruginosa
were resistant to most of the antibiotics tested. Only 50%
of the strains showed sensitivity to imipenem and piperacillin/tazobactam
, while being resistant to ceftazidime , cefepime ,
ceftriaxone , ceftizoxime, gentamicin ,amikacin,
cotrimoxazole , doxycycline , netilmicin, ofloxacin and
aztreonam. . Multiple drug resistance was observed in 86.5% of
isolates from various nosocomial infections.
Discussion :
Infections in orthopaedic patients is an unresolved problem.
Infections occur even though orthopaedicians perform thoroughly
clean procedures during surgery and patients are strictly
managed before and after surgery. According to present results
¸positive cultures were seen in 18.6% of patients, while Akbas
et al11 reported positive cultures in 7.2% of cases.
Mohanty et al12 and Agrawal et al2 have
reported the rate of isolation to be 34% and 53% respectively.
Different institutions have different protocols at the time of
admission to the hospital regarding antibiotic prophylaxis,
which has great influence on relative percentage of isolation of
bacteria. Moreover , the rate of isolation was 18.3% in cases
of fractures which was higher than that reported by Onche et al13
(7.5%). However, other workers have reported it to range between
0.8-13% for both deep and superficial infections. This higher
rate of isolation among the patients of fractures in the present
study may be because of the fact that many of these fractures
were multiple fractures and open fractures which tend to have
higher risk of bone infection due to easy access of bacteria
into the bone, than with closed fractures. Additionally, an
association with severe soft tissue damages in these patients
put them at a higher risk of infection.
However, bacterial growth from patients of osteomyelitis was
relatively less in present study (20%). Results of the current
study show that most frequent nosocomial infections in
orthopaedic patients were SSIs (59.9%) which is higher than
other workers. 13,14 High rates of contaminated,
dirty and trauma related wounds in our study might have
contributed to the high incidence of SSIs. UTIs in the present
study were more common in patients of spinal injury. As
patients of spinal injury are catheterized for longer times, it
increases the chances of UTI in these patients.
Results of our study showed that gram negative infections
continue to be a major threat since gram negative pathogens were
isolated from 75.6% of cases. E. coli remained the most
common pathogen (28.5%) ,followed by K. pneumoniae (25%),
Enterobacter spp. and P. aeruginosa (14.3% each),
Citrobacter spp (10.7%) and A. baumanii (7%).
Agrawal et al2 have reported similar results but
other authors have observed a different spectrum. This may be
due to the fact that type of flora in wards and OTs in different
hospitals vary and also keeps on changing over the years .
E. coli is a commensal of gut and as many orthopaedic
patients are bedridden for prolonged periods, contamination of
wounds, dressing linen, clothes and even hands during perineal
hygiene plays a major role in increasing transmission of
infections. S. aureus was isolated most commonly from
SSIs (7 of 9 isolates of S. aureus) followed by UTI (2 of
9 isolates). Similar results have been reported by Onche et al.13
About 10-30% of healthy people carry this organism in their
nares. Infections by these organisms can also be caused by
patients themselves. Bedsheets, instruments and dressing have
also been found to act as reservoirs of S. aureus.
Antimicrobial resistance pattern of gram-negative bacilli showed
high frequency of resistance to amoxicillin (75-100%),
cephalexin (100%), ceftazidime (62.5-100%), cefepime
(71.4-100%), ciprofloxacin (50-100%), gatifloxacin (62.5‑100%).
Resistance to piperacillin / tazobactam and amoxicillin /clavulanic
acid was (75-100%) each. Carbapenems were found to be most
sensitive drug. The resistance rates as observed in the current
study are similar to those reported by Akbas et al.11
All the strains of P.aeruginosa were resistant to
most of the antibiotics tested. Only 50% of the strains showed
sensitivity to imipenem and piperacillin/tazobactam. High level
of resistance, as observed in the present study, among the
isolates from SSIs may be due to horizontal spread of these
organisms among the patients which may be related to
overcrowding in wards, poor socio economic status, and lack of
hygiene.
It is apparent from the results of antibiograms that
orthopaedics wards and OTs could be a potential reservoir of
nosocomial pathogens. . To control these infections and to
prevent antibiotic resistance, it is suggested that the
committee for controlling infections should be more active and
new antimicrobials should be used with more caution and their
long term use should be discouraged whenever possible.
Summary:
This study has highlighted three main issues in microbiology of
infections in orthopaedic patients. Firstly , the SSIs are the
most important infections in orthopaedic patients, that also
associated with multiple and open fractures. Secondly, gram
negative pathogens dominated in our study. Thirdly , resistant
strains especially among gram negative pathogens have emerged
and that creates problem not only in prescribing post operative
treatment but also in deciding preoperative prophylaxis for such
patients.
Reference :
-
Lynch
P. Infection Prevention with Limited Resources. ETNA
Communications: Chicago
-
Agrawal AC, Jain S, Jain RK, Raza HKT. Pathogenic bacteria in
an orthopaedic hospital in India. J Infect Developing
Countries 2008;2:120-123.
-
Schatzker J. Principles of stable internal fixation. In:
Schatzker J, Tile M (ed). The rationale of operative fracture
care. Spinger-Verlag, Berlin 1996:10-11.
-
Sisk DT. General principles of fracture treatment. In:
Crenshaw AH (ed). Campbell's operative orthopaedics. Mosby,
Missouri 1987:1551-61.
-
Khosravi AD, Ahmadi F, Salmanzadeh S, Dashtbozorg A, Montazeri
EA. Study of bacteria isolated from orthopedic implant
infections and their antimicrobial susceptibility pattern.
2009;4:158-63.
-
Mbamali EI.
Internal fixation of femoral shaft fractures at the Ahmadu
Bello University Teaching Hospital Zaria. Nigerian Medical
Practitioner 1981;2:81-5.
-
Oguachuba HN. Wound
infection in the orthopaedic-traumatology department of Jos
University Teaching Hospital, Jos, Nigeria. Nigerian Med J
1987;17:147-51.
-
Classen
DC, Evans SR, Pestotnik SL. The timing of prophylactic
administration of antibiotics and the risk of surgical wound
infection. N Engl J Med 1992;326:281-5.
-
Collee
JG, Miles RS, Watt B. Tests for identification of bacteria.
In: Collee JG, Fraser AG, Marmion BP, Simmons A, ed. Mackie
and McCartney Practical Medical Microbiology. 14th
ed. New York: Churchill Livingstone 1996.p.131-49,166-167.
-
Bauer AW, Kirby WMM, Sherris JC, Turck M. Antibiotic
susceptibility testing by a standardized single disk method.
Am J Clin Pathol 1966;45:493-6.
-
Akbas A, Bakir M, Savk SO. The examination of nosocomial
infections that develop in the orthopedics clinic. Acta Orthop
Traumatol Turc 1994;28:
-
Mohanty S, Dhawan B, Das BK, Kapil A. Bacteriology of
orthopaedic wound infections in an Indian tertiary care
hospital. Ind J Med Res 2005;121:784-5.
-
Onche II. Post-operative wound infection in implant surgery.
Dissertation submitted to the National Post graduate Medical
Collage of Nigeria. Lagos 2000.
-
Maksimovic J,
Markovic-Denic L, Bumbasirevic M, Marinkovic J, Vlajinac H.
Surgical site infections in orthopedic patients: prospective
cohort study. Croat Med J 2008;49:58-65.
|

