|
Bhaskar Borgohain1,
Praveen Tittal2
1. Department of Orthopaedics & Trauma,
North-Eastern Indira Gandhi Regional Institute of Health and
Medical Sciences, (NEIGRIHMS) Shillong, India.
2.
Department of orthopaedics,
Maulana Azad Medical College, New Delhi
Address for Correspondence:
Bhaskar Borgohain
Asst. Professor and in-charge,
Department of Orthopaedics & Trauma,
North-Eastern Indira Gandhi Regional Institute of Health and
Medical Sciences, (NEIGRIHMS) Shillong, India.Pin:
793018.
Phone :
+91 0364 2538097
Fax :
+91 0364 25380209
E-mail :
bhaskarborg@gmail.com
|
|
Abstract:
Background: Analysis of fracture pattern reveals the amount of
energy imparted to the extremity and alerts the surgeons to
higher risk pattern of injury. Comminuted fractures occur when
the deforming force is a combination of compression, bending and
torsion usually signifying a high energy injury in non-osteoporotic
bone and a high likelihood of severe associated loco-regional
soft tissue injury. Method: The authors present nine consecutive
cases of high energy distal radius fractures in relatively
younger patients, which were associated with severe comminution
with or without an open wound in the metaphyseal area. Results:
These cases of distal radius fractures were roughly falling into
the AO-ASIF type C fractures or Fernandez type V fractures that
signify high energy injuries. All these cases were associated
with other significant skeletal or non-skeletal injuries; either
loco-regional or remote. Conclusion: The author propounds that
severe comminution in the metaphyseal or metadiaphyseal area in
distal radius fractures in relatively younger individuals is an
independent risk factor for associated injuries.
J.Orthopaedics 2010;7(2)e10
Keywords:
Fracture geometry; distal radius; concomitant injuries
Introduction:
Analysis of fracture pattern reveals the amount of energy
imparted to the extremity and alerts the surgeons to higher risk
pattern of injury 1. Comminuted fractures occur when
the deforming force is a combination of compression, bending and
torsion 2. Comminution of bone usually signifies that
there is severe associated loco-regional soft tissue injury. In
osteopenic bone however, comminution may result from low energy
trauma and less soft tissue injury 3. The mechanics
of the fall plays important role in whether a fracture will
occur and which bone will fracture. The orientation of the fall
and location of the impact determine the type of fracture, and
whether a fracture occurs depends on the energy of the fall
(distance to impact and weight of the moving parts) and how much
of that energy is absorbed by protective responses, the impact
surface and soft tissues overerlying the bone 4.
Bones break when the forces applied to them exceed their
strength. The direction of impact is as important as that of the
amount of force itself.5
It is difficult to know how much energy is absorbed by
protective responses, the impact surface and soft tissues over
the bone (covering) before the fracture happens. We feel that
due to protective responses that attempts to prevent vital organ
from injuries; the upper limbs & the body move in unaccustomed
directions or positions and when the bone finally gives way
(fractures) that is the end of protection, so far provided by
the upper limb before loss of weight bearing/transmitting
ability of the limb. At this very point of failure the same
protective process risks injury to other bones and organs. From
a series of cases presenting to the casualty department, we
propose that specific fracture geometry of distal radius in
younger individual not only predicts energy imparted on the
tissue but also may predict existence of associated
loco-regional and even remote injuries.
Materials
and Methods:
The Case series
These cases were noted and recorded over two and a half year
period in a tertiary care hospital.
|
Case No. |
Age
(Years) |
Fracture
(AO) |
Wound
(Gustilo) |
Mode of injury |
Associated injury |
|
1. |
45 |
C3 |
Gr. I |
Fall from height |
# Surgical neck humerus |
|
2. |
50 |
C3 |
Gr. II |
MVA |
Death due to other injury? |
|
3. |
30 |
C2 |
None |
Fall |
2nd MC base # |
|
4. |
11 |
C2 |
None |
Fall from height |
EDH@ |
|
5. |
19 |
C2 |
None |
Fall from height |
Inferior Pubic ramus # |
|
6. |
45 |
C2 |
None |
Fall in stairs |
Dental injury $ |
|
7. |
25 |
C2 |
None |
MVA |
Sup. Pubic ramus # |
|
8. |
22 |
C3 |
Gr.I |
MVA |
Left 5th rib # |
|
9. |
40 |
C3 |
Gr.I |
MVA |
Splenic injury *** |
@ Extradural haematoma
$ Needing tooth extraction
*** With minimum fluid in peritoneum that responded to
conservative treatment.
The first two cases need elaboration. Case no. 1, was a
neglected and heavily contaminated open fracture of distal
radius in 45 year old village lady who fell down from a tree
(Fig 1.) She had a contusion in lower arm which was treated so
far as soft tissue injury. A second fracture was a grossly
displaced ipsilateral surgical neck of humerus proved in X-ray
after admission (Fig 2).

Figure 1:
Case no.1 with metaphyseal extension of fracture line with gross
displacement.
In Case no. 2, this deaf and dumb patient met road side
accident. She had a fracture with unusual comminution (Fig 3).
She was conscious and apparently there were no elements of other
associated injury as per history from her attendants and also on
examination. The fracture was stabilized by external fixator
under local anaesthesia. Immediate postoperative condition was
uneventful, but after 4 hours she became unconscious and had a
cardiac arrest. The possibility of cardiac contusion,
pericardial temponade, head injury or major visceral injury
couldnt be ruled out since autopsy was denied by relatives.

Figure 2:
Case no.1 showing the concomitant missed proximal surgical
neck humerus fracture

Figure 3:
Unusual fracture line in metaphysic in a young adult that
doesnt precisely fall into any common classification

Figure 4:
Another case where comminution is not extensive but fracture
line running into high metaphysis.
Discussion :
These consecutive nine cases of distal radius fractures were
associated with extension of comminution in the high metaphyseal
area with or without comminution in the epiphyseal area. The
metaphyseal extension of fracture line was not always seen in AP
view but may be seen in lateral/oblique view radiograph only.
Osteoporosis was not radiologically apparent in any case. All
these cases were associated with other significant skeletal or
non-skeletal injuries. These fractures were roughly falling into
the type C fractures (especially C3 Type) in AO-ASIF and in
Universal classification of Sarmiento (Fernandez type V
fractures) and they signify high energy injuries.
From this series of cases we propose that fracture geometry of
distal radius in younger individual predicts associated
loco-regional or remote injuries. Our thinking and observation
are based on the fact that effective protective reflexes cushion
the impact of a fall in active individuals. Isolated fractures
of distal radius are classically seen in osteoporotic (but fit)
individuals. But fracture of distal end radius with associated
ipsilateral limb injuries are increasingly found in young
active adult partly due to higher incidence of high energy
trauma and increased participation in sports and similar outdoor
activities 6. Younger individuals are usually
non-osteoporosis and injuries are high energy type. In elderly,
the effective protective reflexes to cushion the impact of a
fall are obtunded corresponding to their age and that is why the
incidence of hip fractures are more common than distal radius
fractures in elderly, which is attributed to increased frailty
and decreased protective response (e.g. rapid reflexive elbow
extension) during a tendency to fall 6.
Theoretically, the longer the length of metaphyseal comminution,
greater is the likelihood of higher energy and higher protective
resistance imparted by the bone of the injured individual and
greater is the likelihood of impact to the surface of collision
at the end point of failure (fracture). Similarly the viscera
and limbs are also likely to get injured at the same time due to
the magnitude of trauma and proximity to the direction of force
(line of fire). The AO-ASIF classification of DER fractures
appreciates the extent or length of metaphyseal comminution
though they recognize articular comminution in more details
since it is more important for DRUJ.
Though many associated injuries in distal radius fractures are
well-described in the literature namely injury to the DRUJ,
triangular fibro cartilage (TFCC), carpal & carpal ligament
injuries, median nerve injury, radial head fracture etc
7-10; no mention is found in these literature about remote
injuries that we have noticed in our cases. The degree of
articular comminution has no correlation with incidence of local
injuries like TFCC injury 10. It is well known that
orthopedic injuries can mask the presence of life-threatening
visceral injuries 11. An open fracture is also known
to dramatize clinical presentation and lead to missed
concomitant injuries.
Associated injuries are important in treatment and for
rehabilitation. We couldnt find any literature mentioning
remote injuries in distal radius fractures. Scapular fractures
are associated with chest injuries, clavicle fractures, rib
fractures, tibial fractures, spleen & liver injuries 12.
But femoral fractures on the other hand are reportedly
associated with other life-threatening injuries 11.
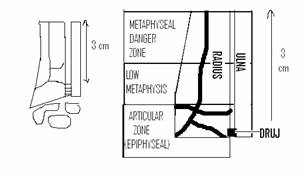
Figure 5:
The proposed metaphyseal danger zone sign. The dark line
depicting the fracture progression line. (DRUJ: Distal Radio-ulnar
Joint.)
Based on these considerations, we propose that metaphyseal
comminution and extension of fracture line approximately 3 cm
beyond the DRUJ may suggest possibility of another unsuspected/
occult injury; remote or loco-regional. Therefore in young
patients this area may be called Metaphyseal danger zone
(Fig.5). If this finding is present we should actively look for
another missed injury. This may be especially true in patients
who are non-cooperative or who have altered sensorium due to
alcohol, drugs or head injuries with a wrist radiograph showing
such fractures or if there is an open wound. Statistical
analysis in a large number of randomly selected cases is needed
to further this observational analysis.
Reference :
-
Claiborne A. Christian In: General principle of fracture
treatment. Canale S.Terry, Editor. Campbells Operative
Orthopaedics. 9th edition, St.Louis: Mosby; 1998:1994
-
Claiborne A. Christian In: General principle of fracture
treatment. Canale S.Terry, Editor. Campbells Operative
Orthopaedics. 9th edition, St.Louis: Mosby; 1998:2004-2006
-
Joseph A. Buckwalter, Thomas A.Einhorn, J.L.Marsh In: Bone and
joint healing. Robert W. Bucholz, James D. Heckman, Charles
Court Brown et al Editors. Rockwood and Greens fractures in
adult. 6th edition, Lippincott Williams & Wilkins; 2006: 304
-
S. R. Cummings, M. C. Nevitt and the Study of Osteoporotic
Fractures Research Group. Non-skeletal determinants of
fractures: the potential importance of the mechanics of falls.
Osteoporosis international. Vol 4, supplement 1, Jan, 1994:
2S67-S70
-
Allan F. Tencer In: Biomechanics of fixation and fractures.
Robert W. Bucholz, James D. Heckman, Charles Court-Brown et al
Editors. Rockwood and Greens fractures in adult. 6th edition,
Lippincott Williams & Wilkins; 2006: 15
-
Prommersberger KJ, Frohner S, Schoonhoven J. Van, Schmitt R.
In: Trauma of the distal forearm. Rainer Schmitt, Ulrich Lanz
editors. Diagnostic imaging of hand. 3rd edition, Stuttgart-Newyork.
Thieme 2008:182
-
Prommersberger KJ, Thomas Pillukat In: Distal radius
fractures. David C. Ring, Mark S Cohen, Editors. Fractures of
the hand and wrist. First edition, Informa Healthcare 2007:
163-165
-
R. Jay French In: Fractures and dislocations of the wrist.
Mark R. Brinker Editor. Review of orthopaedic trauma.
W.B.Saunders, Philadelphia 2001:277-281
-
Harry B. Skinner, Edward Diao, Richard Gosselin, David
Lowenberg In: Musculoskeletal Trauma Surgery. Harry B. Skinner
Editor. Current Diagnosis and Treatment in Orthopedics. Lange
Medical Books/Mcgraw-Hill. 2nd International
Edition 2000: 74-82
-
Bombaci H, Polat A, Deniz G, Akinci O. The value of plain
X-rays in predicting TFCC injury after distal radial
fractures. J Hand Surg Eur Vol. 2008 Jun;33(3):322-6.
-
Adili Anthony Peng, Bhandari Mohit, Lachowski Richard J.et al
.Organ injuries associated with femoral fractures:
Implications for severity of injury in motor vehicle
collisions. The Journal of Trauma: Injury, Infection, and
Critical Care: 46(3)1999: 386-391
-
Weening Brad, Walton Christine; Cole Peter A.; Alanezi Khaled;
Hanson Beate P.; Bhandari, Mohit. Lower mortality in patients
with scapular fractures. The
Journal of Trauma: Injury, Infection, and Critical Care:
Volume 59(6) 2005:1477-1481
|

