|
Abstract:
The authors present a case of a premature neonate, born after
caesarian section, with a distal femoral epiphysiolysis. This
very rare condition can easily go undiagnosed or misdiagnosed
with no pathological findings on conventional X-rays. Using
ultrasonography as a diagnostic tool in this case, timely and
accurate diagnosis was possible, resulting in appropriate
treatment to avoid permanent deformities and dysfunction of the
affected limb.
J.Orthopaedics 2010;7(1)e4
Keywords:
epiphysiolysis; epiphysial fracture; distal femur; neonate.
Introduction:
Distal
femoral epiphysiolysis (DFE) in the newborn infant is a very
uncommon event. This is in contrast to DFE in older children of
which more cases have been reported. Over the past 50 years,
only 8 reports, with 11 cases of DFE in the newborn child have
been described in European and American literature. [1-8] We
present a case of neonatal distal femoral epiphysiolysis and
describe the use of ultrasonography as a diagnostic tool.
Case Report:
A male patient, weighting 1730g, was born at 31+2
weeks pregnancy by caesarian section. After preterm broken
membranes, oligohydramnion caused fetal distress which initiated
the preterm operative delivery. On day one after birth, the
premature neonate presented with minor spontaneous movement (pseudoparalysis)
of the right leg. Physical examination showed a red and
edematous right upper leg with both right knee and hip
maintained in flexion. On palpation of the femur and with
passive motion of the leg, visible discomfort was obvious. On
conventional X-rays, there were no evident signs of fracture
visible, besides the presence of a minimal metaphyseal avulsion
fragment at ventral side of the distal femur (figure 1).

Figure 1:
Lateral
and anteroposterior X-ray of the right leg showing a minimal
metaphyseal avulsion fragment on ventral side of the distal
femur.
Because
of the clinical findings ultrasonography was performed, showing
severe ventrally dislocation of the right distal femoral
epiphysis with periostal hematoma (figure 2 and 3).
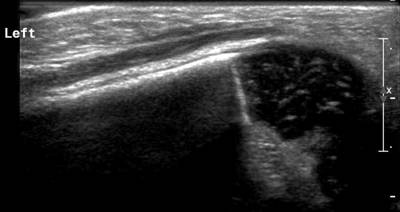
Figure 2:
Ultrasonography of the left femur showing normal distal
epiphysis.
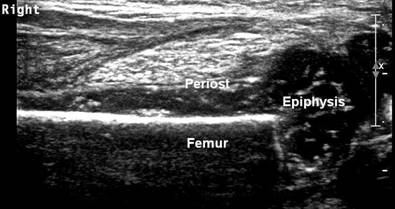
Figure 3:
Ultrasonography of the right femur showing periostal hematoma
and ventrally displaced distal epiphysis with intact periosteum
and perichondrium.
The
diagnosis DFE was made. Manual reposition of the epiphysis with
ultrasonographic control was not possible 4 days after birth.
Therefore, a conservative treatment was initiated with a plaster
cast for comfort during 1 week. Ultrasonographic control showed
no progression of dislocation. At 3 weeks after birth, a control
X-ray was made, showing diffuse callus formation around the
distal femur (figure 4).

Figure 4: Lateral and anteroposterior X-ray of the right leg
3 weeks after birth showing diffuse callus formation around the
distal femur.
The
cause of the epiphyseal dislocation in this case remains
uncertain. Since there was no callus formation on the X-rays,
and movement of the fracture while performing ultrasonography 4
days after birth, it is unlikely that the fracture was older
than 1 week. The X-rays made at 3 weeks after birth, showing
evident callus formation, confirm this hypothesis. Therefore,
the fracture was most likely due to a trauma during operative
delivery or shortly after birth. In available literature,
neonatal DFE has been reported as a complication of delivery.
[2,3,4,6,7] Risk factors for obstetric bone injuries in general
include malpresentation often leading to obstructed labour,
operative deliveries and lack of antenatal care. [9] In this
case there was a normal presentation and good antenatal care.
However, because of the oligohydramnion, the fetus could have
been entrapped in the uterus causing a problem during operative
delivery. A cause postpartum is very unlikely because the
patient was admitted to the neonatal intensive care unit with
constant monitoring.
Discussion :
Distal
femoral epiphysiolysis in the newborn infant is a very uncommon
event. This suggests that the condition is being underdiagnosed.
Little is known about the consequences of this condition in the
newborn child. However, in older children epiphyseal fractures
of the distal femur have a high incidence of complications,
particularly of growth arrest, and treatment favors a
conservative approach. [10,11]
Diagnosis of a DFE in the newborn may be difficult with clinical
signs of inflammation and can be missed easily on conventional
X-rays because the bone matrix in neonates consists of large
amounts of cartilage. Therefore, the condition can go
undiagnosed or misdiagnosed as septic arthritis, osteomyelitis,
paralysis or lymphedema, without appropriate treatment. But
still, with no findings on X-rays, there should be a high index
of suspicion for this condition.
Other
methods than ultrasonography to diagnose epiphysiolysis in
neonates are MRI, joint aspiration that reveals haemarthrosis
and the presence of fat glubules, and arthrography that shows
the displacement of the epiphysis on the metaphysis.
Ultrasonography however, is a rather fast, easy to use, patient
friendly and cheap diagnostic tool. Because of its ability to
visualize the nonossified skeleton in neonates, its dynamic
capabilities, its accuracy, and its lack of nonionizing
radiation, it has been widely utilized for several decades in
pediatric orthopaedics in the diagnosis and follow-up of hip
dysplasia. [12] Furthermore, ultrasonography of the distal
femoral epiphysis in particular, is considered as a useful and
reliable bedside tool for the assessment of skeletal maturity in
newborns. [13]
Conclusion:
We
present a case of a premature neonate, born after caesarian
section, with a distal femoral epiphysiolysis. This rare
condition can easily go undiagnosed or misdiagnosed with no
pathological findings on conventional X-rays. Recognition by
using ultrasound allows timely and accurate diagnosis and
appropriate treatment, avoiding permanent deformities and
dysfunction of the affected limb.
Reference :
-
Fracture-separation of the distal femoral epiphysis in a
premature neonate. Eliahou R, Simanovsky N, Hiller N,
Simanovsky N. Journal of Ultrasound in Medicine. 2006
Dec;25(12):1603-5
-
Epiphysiolysis in the distal femur as a birth injury in
Cesearean section. Trier H.
Ugeskr
Laeger. 1992 May 25;154(22):1574-5 Article in
Danish
-
Bilateral distal femoral epiphyseal fractures following home
delivery: a case report. Journal of the Arkansas Medical
Society. 1988 Feb;84(9):364-6.
McCollough FL,
McCarthy RE.
-
Traumatic separation of the distal femoral epiphysis in the
newborn. Banagale RC. Kuhns LR. Journal of Pediatric
Orthopedics. 3(3):396-8, 1983 Jul.
-
Traumatic separation of the epiphysis of the lower end of the
femur.
Padovani JP,
Rigault
P,
Raux P,
Lignac
F,
Guyonvarch G.
Rev
Chir Orthop Reparatrice Appar Mot. 1976
Mar;62(2):211-30. Article in French
-
Obstetrical detachment of lower femoral epiphysis.
Monteleone M,
Scillone GB,
Cristiani G.
Clin
Ortop. 1974 Apr-Jun;25(2):75-83 Article in
Italian.
-
Typical
obstetric epiphysiolysis of the distal humeral epiphysis in a
newborn infant. Bumbic S. Srpski Arhiv Za Celokupno
Lekarstvo. 98(11):1341-5, 1970 Nov. Article in Serbian
-
Neonatal distal femoral physeal fracture requiring closed
reduction and pinning. Mangurten HH, Puppala B, Knuth A.
Journal of Perinatology. 2005 Mar;25(3):216-9
-
Bone
injuries during delivery.
Bhat BV,
Kumar A,
Oumachigui A.
Indian
J Pediatr.
1994 Jul-Aug;61(4):401-5.
-
Predicting the outcome of Physeal Fractures of the Distal
Femur. Arkader et al. Journal of pediatric orthopaedics.
2007 Sept 27(6), pp 703-708.
-
Fractures of the distal femoral epiphyses. Factors influencing
prognosis: a review of thirty-four cases.
J Bone
Joint Surg Am.
1977 Sep;59(6):742-51.
Lombardo SJ,
Harvey
JP Jr.
-
Hip ultrasound. Bancroft LW, Merinbaum DJ, Zaleski CG,
Peterson JJ, Kransdorf MJ, Berquist TH. Seminars in
Musculoskeletal Radiology. 2007 Jun;11(2):126-36
-
Ultrasonographic assessment of bone maturity in newborns.
Leshem E. Bialik V. Hochberg Z. Hormone Research.
57(5-6):180-6, 2002.
|

