|
Abstract:
We present a 4 month old male who presented with a pre-tibial
soft tissue mass with cortical destruction found in the
juxtapyseal metaphysis found to represent Langerhans cell
histiocytosis (LCH). Eccentric, cortically based LCH may be
under-appreciated unless they occur in regions with little
overlying soft tissue, such as the calvarium and anterior calf.
Pre-tibial LCH should be included in the differential diagnosis
of a pre-tibial mass, and cross-sectional imaging is critical in
distinguishing LCH from the more common entities such as pre-tibial
subcutaneous granuloma annulare.
J.Orthopaedics 2010;7(1)e2
Keywords:
Langerhans Cell Histiocytosis, Magnetic resonance imaging,
tibia, Pediatric imaging, Radiography
Introduction:
The most common pathologically proven pre-tibial mass in a child
is subcutaneous granuloma annulare. We present an unusual case
of pre-tibial Langerhans cell histiocytosis (LCH). Eccentric LCH
may be under-appreciated unless they occur in areas with little
overlying soft tissue such as the calvarium and anterior calf,
and cross-sectional imaging is critical in distinguishing LCH
from subcutaneous granuloma annulare and other tumor and
tumor-like conditions in children affecting the anterior tibia.
Case Report:
A 4-month-old male presented to his pediatrician after the
parents noticed a pre-tibial mass over the left proximal tibia.
The mass was nonmobile and without erythema, warmth, or
tenderness. Initial workup included radiographs, which were
normal. This was followed by an ultrasound, which demonstrated
a hypoechoic, soft tissue mass with cortical destruction (figure
1). CT imaging demonstrated a 5mm eccentrically located lucent
lesion in the proximal tibial metaphysis with cortical
destruction and a soft tissue mass (figure 2). MR imaging
demonstrated an intraosseous lesion with a large anterior
exophytic soft tissue component within the juxtaphyseal
metaphysis with undercutting of the physeal equivalent region of
the tibial tuberosity. The lesion was isointense on T1W images
and hyerintense on T2W images with subtle enhancement as well as
anterior periosteal rim enhancement (figures 3). Open biopsy
with frozen section analysis, and subsequent curettage of the
lesion, showed histiocytes with grooved, folded, indented nuclei
and thin nuclear membranes without atypia in a background of
scattered small lymphocytes, macrophages, eosinophils, and a few
giant cells (figure 4).
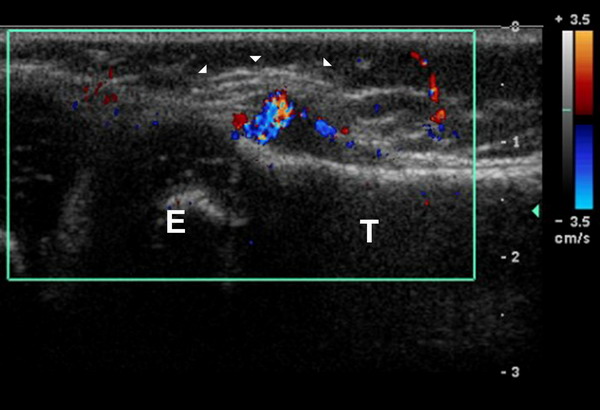
Figure 1: Grey Scale with Color Doppler Longitudinal
Ultrasound image demonstrates a hypoechoic pre-tibial soft
tissue lesion (white arrowheads) with central color flow (T
tibial shaft, E tibial epiphysis).
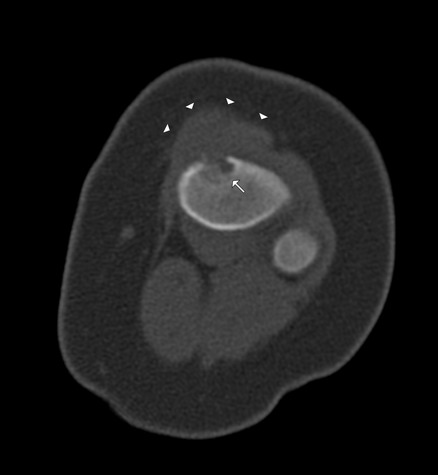
Figure 2: Axial CT image through the proximal tibia
demonstrates anterior lytic lesion with minor intramedullary
extension (white arrow) with significant pretibial soft tissue
component (white arrowheads).
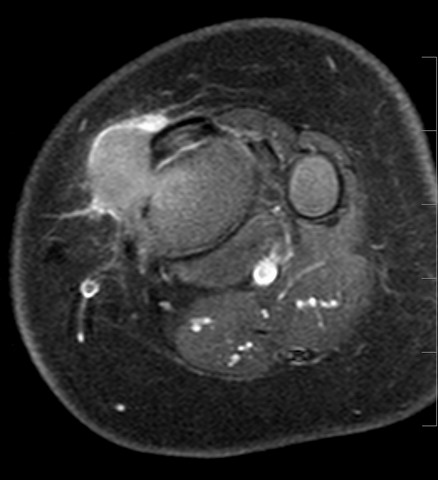
Figure 3: Axial fat saturated T1 post-contrast images
demonstrate subtle central enhancement and anterior rim
enhancement of the pre-tibial mass.
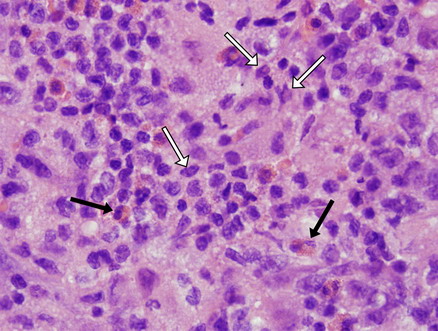
Figure 4: Hematoxylin and eosin (H & E) stain of the
cortical lesion shows multiple abnormal histiocytes (white
arrows) with grooved, folded, indented nuclei and thin nuclear
membranes without atypia in a background of eosinophils (black
arrows).
Immunohistochemical staining demonstrated multiple S-100
positive cells, which are characteristic of Langerhans cells,
and therefore LCH was the diagnosis. CT imaging of the chest
and abdomen as well as bone scintigraphy demonstrated no other
foci of disease. Curettage was considered therapeutic, and the
patient remains asymptomatic without evidence of new lesions or
recurrence. The patient has been disease free for approximately
3 months at the time this report was written.
Discussion :
Langerhans cell histiocytosis (LCH) which was formally known as
Histiocytosis X, is a rare disorder which may manifest with
either local or systemic effects, most commonly affecting male
(2:1) children younger than 15.1 Histology consists
of unusual monocyte-like cells called Langerhans cells, which
have vesicular, grooved nuclei. These cells are usually seen in
a background of eosinophils and this combination is unusual in
pathologic specimens other than LCH.
Up to 80% of the LCH lesions that occur in children are isolated
to bone.1,2 Local pain is the primary symptom and
sometimes a palpable tender mass may be present.3
The osseous manifestations of LCH present more than 50% of the
time as solitary, lytic lesions that are moderately destructive
and involve the flat bones of the skull, mandible, ribs, and
pelvis and most commonly affect children 1-3 years of age.2,4
Less commonly the long bones of the appendicular skeleton are
involved, with lesions most commonly occurring in the diaphysis
(58%), followed by the metyphysis.5 Physeal and
epiphyseal involvement is rare. The lesions of the appendicular
skeleton most commonly present as a centric lesion with
endosteal scalloping.5 Eccentric, cortically based
lesions may be a more common finding than has been reported in
the literature. When LCH involves cortex where there is little
overlying soft tissue, such as the calvarium, or the anterior
tibia, as seen in our case, they are probably detected at an
earlier stage because they can be readily palpated compared with
osseous lesions surrounded by more substantive soft tissue, such
as the mid-diaphysis of the femur.
The top differential clinical consideration of a pre-tibial mass
in a child was subcutaneous granuloma annulare, but this was
excluded as a consideration given the presence of cortical
destruction of the anterior tibia. The alternative differential
diagnostic considerations for this patients pre-tibial mass
given the imaging findings of anterior cortical destruction
included subacute osteomyelitis with mass-like granulation
tissue, an unusual manifestation of a solid osteofibrous
dysplasia or adamantinoma with anterior cortical breech, Ewings
sarcoma, leukemia/lymphoma, and cortically based solid
aneurysmal bone cyst. Cross sectional imaging work-up in this
patient was helpful in defining the lesion epicenter and the
extent of cortical and intramedullary destruction, planning the
biopsy and operative treatment, and excluding diagnostic
considerations such as cortical aneurysmal bone cyst or an
unusual manifestation of infection.
Treatment of patients with isolated LCH of the appendicular
skeleton typically consists of curettage of the affected site
with possible use of allograft bone if there is concern for
pathologic fracture at the site of curettage. Asymptomatic
lesions may be managed conservatively as the lesions commonly
regress and heal with time. Systemic involvement may require
treatment with chemotherapy and/or radiation.2,4 Our
patient underwent curettage of the lesion and is currently
asymptomatic with no other lesions identified.
In summary, cortically based LCH presenting with a palpable soft
tissue mass is an unusual manifestation in long bones, although
a frequent finding affecting the calvarium. Cortically based LCH
may in fact be more common than what has been reported in the
literature and may represent an early manifestation of osseous
LCH. Cortically based LCH lesions of the long bones are
under-appreciated unless they occur in areas with little
overlying subcutaneous tissue, such as the anterior calf. In
the proper clinical context and patient age, LCH should be a
diagnostic consideration in children presenting with a pre-tibial
mass, which ultimately requires biopsy to differentiate from
other neoplastic and tumor-like cortically based lesions in
children.
Reference :
-
Azouz MA, Saigal G, Rodriquez MM, Podda A. Langerhans cell
histiocytosis: pathology, imaging and treatment of skeletal
involvement. Pediatric Radiology 2005; 35:103-115.
-
Hoover KB, Rosenthal DI, Mankin H. Langerhans cell
histiocystosis. Skeletal Radiol 2007; 36:95-104.
-
David R, Oria RA, Kumar R, et al. Radiologic Features of
Eosinophilic Granuloma of Bone. AJR Am J Roentgenol 1989;
153:1021-1026.
-
Meyer JS, Harty MP, Mahboubi S, et al. Langerhans cell
histiocytosis: presentation and evolution of radiologic
findings with clinical correlation. RadioGraphics 1995;
15:1135-1146.
-
Levine SM, Lambiase RE, Petchprapa CN. Cortical lesions of
the tibia: characteristic appearances at conventional
radiography. RadioGraphics 2003; 23:157-177.
|

