|
1Nobuyuki Kumahashi, 1Kohei
Naitou,1Michihaya Kohno, 1Masatoshi
Tobita, 1Kazushi
Nishimura,
2Yuji Uchio.
1Department of Orthopedics,
Ohda
Municipal
Hospital
, 1428-3 Yoishinaga, Ohda, Ohda-shi, Shimane 694-0063,
Japan.
2Department of Orthopedics, Shimane University School of
Medicine, 89-1 Enya-cho, Izumo-shi, Shimane 693-8501,
Japan.
Address for Correspondence:
N. Kumahashi
Department of Orthopedics,
Ohda
Municipal
Hospital
,1428-3
Yoishinaga, Ohda, Ohda-shi, Shimane 694-0063,
Japan.
Phone: +81-854-82-0330
Fax : +81-854-84-7749
E-mail:
n-kuma@med.shimane-u.ac.jp
|
|
Abstract:
We
report successful use of navigation-assisted screw fixation for
an acetabular fracture. Our patient was a 52-year-old man who
was in a motor vehicle accident, sustaining an open patella
vertical fracture and minimally displaced acetabular fracture
following posterior hip dislocation. First, we arthroscopically
repaired the patellar fracture with three cannulated cortical
screws. We fixed the acetabular fracture with percutaneous
fluoroscopic navigation assistance employing a 30-mm long
cannulated cancellous screw. Bone union of the acetabulum was
achieved three months after surgery, and the screws were removed
nine months after the operation. No intraoperative
complications, including nerve injury or bleeding, occurred.
No radiographic evidence of secondary fragment
displacement or degenerative changes has been observed for
follow-up forty months. This patients satisfactory
clinical outcome showed that percutaneous screw in situ fixation
using a navigation system was a safe and minimally invasive way
to treat this stable type of acetabular fracture.
J.Orthopaedics 2009;6(2)e5
Keywords:
acetabular
fracture; minimally invasive fixation; navigation-assisted
surgery
Introduction:
Posterior
wall fracture, the most common form of acetabular fracture, is
often caused by high-energy trauma. The most important treatment
for acetabular fracture is exact reduction of the acetabular
dome, rigid fixation, and early rehabilitation 1.
Acetabular fracture is traditionally approached with
conservative treatment; however, it is well known that 1 to 2 mm
of displacement in reduction can lead to secondary
osteoarthritis 2,
3.
Recently,
surgery has become the gold standard treatment in cases of
fragment displacement greater than 2 mm or fractures involving
the weight-bearing dome 2,
3. Surgical treatment of pelvic and acetabular fractures
is technically difficult, even with percutaneous pelvic
fixation, because of the great care needed to minimize risk of
injury to the intrapelvic organs and neurovascular bundles.
Image intensification is mandatory during percutaneous pelvic
surgery to insert screws accurately and reduce intraoperative
complications. Consequently, radiation exposure is increasing
for both
patients
and surgical staff 4. Safe and accurate insertion of
percutaneous screws requires fluoroscopy or three-dimensional
reconstruction computed tomography (CT) scans with a
computerized navigation system
5,6,7,8.
Several computer navigation systems have been
developed to improve the accuracy of aligning the components in
total hip and knee replacement.
Some studies indicate that navigational assistance
improves alignment accuracy compared with conventional
techniques 9,10. Navigation
systems have also facilitated treatment of acetabular fractures 5,
7,8.
We
present a successful case of fluoroscopic navigation-assisted
percutaneous screw in situ stabilization of a posterior-wall
acetabular fracture after posterior dislocation.
Case
Report:
A
52-year-old man who was injured in a car accident presented with
right knee pain and right hip pain. There was an open patella
fracture (GustiloⅠ) and an acetabular fracture (62 A1, AO
classification, 3x2cm) secondary to posterior hip dislocation
(Fig.1). On the day of injury, we repaired the right knee
arthroscopically using three (length, 46, 48 and 50 mm)
cannulated cortical screws; this was done under lumbar
anesthesia. Four days after the first procedure, we
osteosynthesized the posterior-wall acetabular fracture using
navigation assisted surgery under lumbar anesthesia. Briefly,
the patient was placed supine on a traction table. The
injured leg was positioned in neutral position. The other leg
was positioned in 90° flexion and 30° abduction so we could
easily use a C-arm. In this case, since the minimal
displacement (1 mm) of this fracture meant that we did not need
to perform a reduction procedure, we used the navigation system
for arthroplasty to assist percutaneous in situ fixation.
A single patient tracker pin (4 mm diameter) for the Stryker
Imageless Navigation System (Stryker® LEIBINGER,
Kalamazoo
,
MI
) was inserted into the right anterior superior iliac spine
through a 1.5-cm skin incision. Four preliminary
fluoroscopic views (anteroposterior, lateral, and bilateral
oblique views) were then obtained and calibrated into the system
for placement of implants. The views were displayed
simultaneously, and the ideal trajectory was chosen on all four
views to verify safe screw placement (Fig.2). After satisfaction
with an adequate direction for insertion of the drill pin, a
1.5-cm long skin incision was made and a drill guide pin
(diameter, 1.6 mm) was passed according to the navigated line.
The pointer was easy to put into the posterior hole of the drill
reamer, and we could see the exact navigated blue line during
drilling. Prior to insertion of the cannulated screw, the
position of the guide wire was verified by fluoroscopy. A 4.0 mm
cannulated cancellous screw (length, 30 mm) (ACE Japan Medical
Dynamic Marketing, INC.,
Japan
) was passed over the drill guide after overdrilling. A
single screw fixation was the limitation of this case because of
the small fragment (3x2cm). Fixation was tightened, the
guide pin was removed, and skin was sutured with Manipular after
washing with saline (Fig.3). There was almost no bleeding. The
fluoroscopic time was 1 minute and operative time was 57 minute.
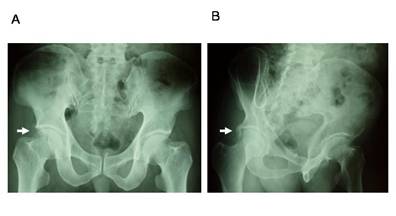
Figure
1: Preoperative X-ray films.
White arrows indicate the fracture line.
(A)
anteroposterior view. (B) oblique view.

Figure
2: Screen display as seen intraoperatively during screw
insertion. The
position of the drill guide (in blue) is presented
simultaneously on all four views to determine optimal trajectory
for placement of the cannulated screw. The blue line indicates
the virtual track of the guide wire. The fracture line is best
seen in view (A). (A)R-oblique view. (B) anteroposterior view
(C)lateral view (D)L-oblique view.
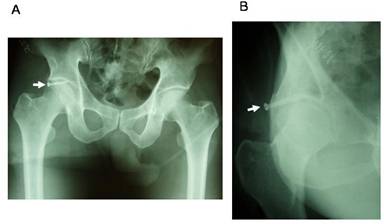
Figure
3: Postoperative X-ray films. White
arrows indicate the cannulated cancellous screw.
(A) anteroposterior view. (B) oblique view.
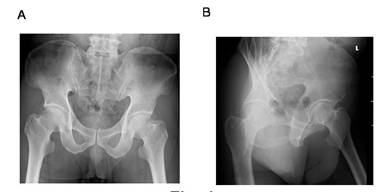
Figure
4: Postoperative X-ray films (forty months after operation)
following removal of the
cannulated cancellous screw.
(A)
anteroposterior view. (B) oblique view.
Continuous
passive motion was started two weeks after hip repair.
Partial weight bearing was allowed at four weeks.
Full weight bearing was started at six weeks.
Xp
and CT imaging showed bone union three months postoperatively.
Subsequently, the screw head of the patella screw became
painful, requiring its removal. Although we explained to the
patient that the hip screw did not require removal, the patient
elected to have both the knee and hip screws removed nine months
after the operation.
During forty months of follow-up, no intraoperative or
postoperative complications including neurological defects,
infection, osteonecrosis of the femoral head, fragment
displacement, screw failure, or degenerative changes have
occurred (Fig 4). We rate the clinical outcome as satisfactory.
Discussion :
Several
reports of navigation-assisted fixation of acetabular fractures
have been published. Crowl reported a series of nine patients
with anterior column acetabular fractures who underwent
percutaneous fixation using a virtual fluoroscopy surgical
navigation system by Medtronic 11. Clinical results
were excellent, and there was a low degree of concern regarding
anticipated late complications. Mosheiff reported on the
percutaneous insertion of 45 cannulated screws in 29 patients
(AO:61B1,2,3 C1,2 62A2,3 B1,2,3) with pelvic and acetabulum
fractures, using a computerized fluoroscopic navigation system
by Medtronic
7. Their accuracy of screw placement was 2 mm and 5°.
Since 2002, we have been using the Stryker Imageless Navigation
System in total knee arthroplasties and in the treatment of
greater trochanteric fractures, and the accuracy of its system
have been proved 9,10. In
the case report presented herein, because the fragment was small
(3x2cm) and minimally displaced (62A1, AO classification),
reduction was not needed. Although this case might have
been considered to fall outside of the range of indications for
surgery, because the fracture involved the posterior wall and
because the patient was middle-aged, we felt that surgical
fixation was indicated in order to maintain the stability of the
joint and prevent post-traumatic osteoarthritis
2,3. Use of the Navigation System not only
facilitated accurate single screw fixation of the fracture
fragment, but it also enabled us to treat the injury in a
minimally-invasive manner by allowing us to forgo plating, which
is the customary treatment for such injuries, helping us to
achieve a good clinical result. Had the displaced fragment
required reduction, open reduction and rigid fixation of the
fragment by plating would have been necessary.
There
are some advantages of fixation of acetabular fractures using a
navigation system. First, conventional methods involve
high-radiation dosages for both patient and surgical staff. Use
of navigation systems can reduce intraoperative radiation
exposure (1minute). Second, this technology can reduce operative
time (57 minutes). Third, the procedure was minimally invasive
and bleeding loss was almost nonexistent. In our patient, only
two 1.5-cm skin incisions were required, and pain was reduced
postoperatively.
In
a study by Carmack et al. analyzing errors in detecting
inappropriate screw insertion using intraoperative fluoroscopy
versus computed tomography, the authors noted that
intraoperative fluoroscopy has the advantage of enabling
intraoperative diagnosis of intra-articular screw penetration 12.
In our case, we used four preliminary fluoroscopic views
simultaneously during our fixation of a small bone fragment.
None of the postoperative CT slices showed penetration of the
acetabular dome, thereby confirming adequate fixation.
Percutaneous
screw in situ fixation under fluoroscopic guidance proved to be
a safe technique for treating our patients stable acetabular
fracture that did not require reduction of the small bone
fragment. Our
success suggests that percutaneous fixation under a navigation
system also might be useful for treating non-displaced fragments
resulting from other kinds of fractures.
Reference :
-
Helfet
DL, Borrelli J, Di Pasquale T, Sanders R. (1992)
Stabilization of acetabular fractures in elderly patients. J
Bone Joint Surg Am;74:753-765.
-
Letournel
E, Judet R (1993) Fractures of the acetabulum 2nd ed.
Springer Verlag, Berlin.
-
Matta
JM, Anderson LM, Epstein HC (1986) Fractures of the
acetabulum. A retrospective analysis. Clin Orthop
205:230-240
-
Sanders
R, Koval KJ, DiPaquale T, Schmelling G, Stenzler S, Ross E.
(1993) Exposure of the orthopaedic surgeon to radiation. J
Bone Joint Surg Am 75:326-330
-
Grützner,
PA Rose E, Vock B (2002) Computer-assisted screw
osteosynthesis of the posterior pelvic ring.
Initial experiences with an image reconstruction
based on navigation system UnfallchirurgMar;105(3):254-260
-
Mouhsine
E, Garofalo R,
Borens O, Wettstein M, Blanc CH, Fisher JF, Moretti B,
Leyvraz.PF (2005) Percutaneous retrogradescrewing for
stabilisation of acetabular fractures. Injury
36(11):1330-1336
-
Mosheiff
R, Khoury A , Weil Y, Liebergall M (2004) First generation
computerized fluoroscopic navigation in percutaneous pelvic
surgery. J Orthop Trauma Feb;18(2):106-111
-
Stuckl
U, Konig B, Dahne M, Raschke M, Hass N. (2002)
Computer assisted pelvic and acetabular surgery. Clinical
experiences and indications.Unfallchirurg
Oct;105(10):886-89
-
Sparmann
M, Wolke B, Czupalla D Banzer D (2003) Positioning of total
knee arthroplasty with and without navigation support. J
Bone Joint Surg Br 85:6:830-835
-
Stuckl
B, Nogler M, Rosiek R, Fisher M, Krismer M, Ksssler O.
(2004). Navigation improves accuracy of rotational
alignment in total knee arthroplasty. Clin Orthop
426:180-186
-
Crowl
AC, Kahler DM (2002) Closed reduction and percutaneous
fixation of anterior column acetabular fractures. Comput
Aided Surg 7(3):169-178
-
Carmack
DB, Moed DH, McCarroll K, Freccero D. (2001) Accuracy of
detecting screw penetration of the acetabulum using
intraoperative fluoroscopy and computed tomography. J
Bone Joint Surg Am 83:1370-1375.
|

