|
Abstract:
Isolated
solitary intramuscular cysticercosis without involvement of
central nervous system is a rare entity. We present a case of
solitary cysticercosis of deltoid muscle in a 14 year old
vegeterian child who presented with features of focal myositis
without any systemic or neurological manifestation.
J.Orthopaedics 2009;6(2)e11
Keywords:
Cysticercosis;
Intramuscular cysticercosis; Deltoid muscle; Magnetic resonance
imaging
Introduction:
Cysticercosis
is no longer an endemic disease of the developing countries
only. It is a global problem, because of the influx of
immigrants from endemic areas1,2. The encysted tape
warm larva can lodge in subcutaneous tissues, muscles, eyes,
nervous system and many other organs of human body leading to
variable presentation. Most soft tissue and muscular cysticercal
affection is associated with central nervous system involvement
or multiple cysts1-7. Solitary cysticercosis of
muscle without involvement of central nervous system is a rare
entity and there are few sporadic handfuls of case reports in
the literature2,3,5,6,8-11. It causes diagnostic
dilemma as there is lack of specific features. We present
a case of solitary intramuscular cysticercosis in a 14 year
vegetarian child involving the right deltoid muscle, where the
diagnosis was established by magnetic resonance imaging.
Case Report:
A
fourteen year male child presented to us with pain and swelling
over the lateral aspect of proximal right arm. He had history of
trauma over the site by one of his friend with wooden scale in
his classroom one day back. . The swelling was soft, diffuse,
erythematous and mild tender. There was mild increase in
temperature of the local part. The child was advised local and
systemic anti-inflammatory medication for the same. Even after 3
weeks of trauma, the swelling did not show any sign of
resolution. Radiograph of the local part revealed soft tissue
swelling with out any bony injury (Fig 1). The parents
were consolated that it may take another few weeks for
resolution considering the entity as post traumatic muscle
contusion. The patient came back to us with similar complaint
even after 6 weeks. Ultrasound of the right arm showed an
intramuscular hypoechoic area of size 1.6 x 0.7x 0.5 cms
involving the superior part of right deltoid muscle. The
radiologist gave the possible diagnosis of liquefied hematoma or
an inflammatory lesion. It is not uncommon to find tubercular
pyomyositis or a cold abscess with such presentation
particularly in India. Considering the above history and
sonography findings cold abscess of right deltoid was suspected.
Hematological parameters showed normal complete blood count. But
the eosinophil count (eosinophil 16) was raised. With absence of
contact history, systemic signs or symptoms, normal chest
radiography and most importantly negative tuberculin test;
tuberculosis was excluded. However MRI of the local part
was advised before proceeding for aspiration cytology. Right
deltoid muscle showed small oval cystic foci of T2
hyperintensity and T1 hypointensity measuring 6x5 mm in size
(Fig 2). It was found to be oriented along the direction of
deltoid muscle fibers (Fig 3a). A sorrounding area of illdefined,
T2 hyperintensity measuring 2.6X 2.4 cm was seen suggestive of
edema or inflammatory changes. The central hyperintense foci
shows peripheral contrast enhancement in post contrast images.
Perilesional contrast enhancement was also seen (Fig 3b).
Intermuscular fascia also showed evidence of hyperintensity and
enhancement. Adjacent subcutaneous fat was normal. Ipsilateral
humerus showed normal cortical and marrow substances. The image
finding reliably established it to be intramuscular
cysticercosis. The child had no history of seizures or
neurological abnormalities and no neurological or systemic
abnormalities were elicited on physical and radiological
examination. Patient was put on oral antihelmithic drug
albendazole (15mg/kg) for 4 weeks. Along with that NSAID was
advised for few days. After completion of the treatment, the
swelling had completely subsided without any residual
complication.
Fig
1. X-ray of right arm AP view shows the soft tissue swelling, no
bony or intraarticular pathology appreciable
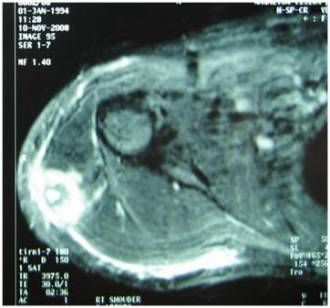
Fig
2. MRI of right arm with shoulder joint shows a small cystic
focus in the right deltoid muscle (T2 hyperintensity),
perilesional T2 hyperintense image suggest the edema or
inflammatory changes

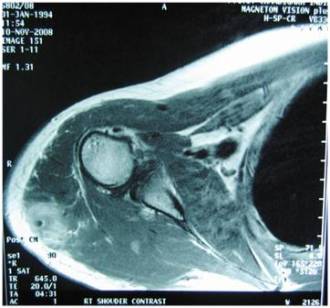
Fig
3a and b. Coronal and transverse cut section of MRI show
peripheral contrast enhancement in post contrast images around
the central hyperintense focus. Perilesional contrast
enhancement is also seen. Intermuscular fascia also shows
evidence of hyperintensity and enhancement. Adjacent
subcutaneous fat is normal. Note should be made that the
orientation of the cystic lesion is along the direction of
muscle fibre
Discussion :
Cysticercosis
occurs when a person ingests pork tapeworm eggs (not the
larvae), usually by consumption of raw or undercooked pork,
fecally contaminated water, or vegetables. The eggs hatch in the
intestine and develop into larvae that penetrate the intestinal
wall and invade various organs and tissues of the body. Human
cysticercosis is caused by this encysted larva of the tapeworm Taenia
solium. It can lodge anywhere in the human body but
subcutaneous tissues, muscles, eyes and nervous system are more
commonly affected1,2,4,5,7,10. Children are commonly
affected because of increased chances of fomite infection5.
Cysticercosis
is common in Mexico, Central and South America, Africa, India,
China, Eastern Europe, and Indonesia. Infection is very rare in
travelers but not uncommon in immigrants from Solitary muscular
and soft tissue cysticercal involvement is a rare disease per se
and it has been used as a marker of neurocysticercosis.
Therefore, central nervous system or ocular involvement should
be ruled out if systemic involvement is suspected1-7.
The intramuscular cyst may remain asymptomatic for a
long time and finally disappear quietly; rarely do they calcify.
In very rare situation as in the present one; they become
inflamed and manifest as a growing area of redness, edema and
pain. Inflammation of the tissue suggests death or degeneration
of the parasite with leakage of the antigens and cellular
response of the body4,7. In this case the cyst wall
might have ruptured because of trauma and the antigens inside
the wall have leaked into the surrounding area inciting an
inflammatory reaction. Three types of clinical manifestations of
muscular cysticercosis have been described: the myalgic,
myopathic type; the nodular or masslike type4. Our
patient had the mass like type presentation, which simulate
benign neoplastic conditions of muscles or an intramuscular
abscess.
As
per the literature laboratory studies in the form of complete
blood count and liver function test may not contribute in
diagnosis; as they are nonspecific. The WBC count is usually
with in normal range and most patients do not have eosinophilia
unless the parasitic antigen is leaking into the surrounding
tissue and evoke an inflammatory reaction7,12. The
increased eosinophil count in the present case provided adequate
hint about helmenthic infection. Because of its atypical
presentation, however a diagnosis of cold abscess was made
initially. MRI of arm showed it to be a cystic ring enhancement
lesion and diagnosis of cysticercosis was made.
The
differential diagnosis of muscular cysticercosis includes
lipomas, epidermoid cysts, neuroma, neurofibromas, pseudoganglia,
sarcoma, myxoma, pyomyositis or tuberculous lymphadenitis2,3,5.
Plain radiographs rarely show cysticerci except in chronic cases
when they calcify. These oval or ellipsoid masses typically lie
in the direction of muscle fibres. However, in most cases,
high-resolution sonography can facilitate the diagnosis of
muscular cysticercosis. Computed tomography and MRI scans are
the other modalities used for imaging muscular cysticerci,
showing their location, number, and relationship to the
surrounding structures1,2,4,5,7. The diagnosis in the
case reported here was first suggested on the basis of MRI
findings. MRI can sometime shows charecteristic appearance of
solitary cysticercosis and a scolex within. However ultrasound
could not contribute in making the diagnosis in this case, as it
is highly operator dependent. MRI clearly showed a cyst
with hyperintensity in T2 weighted image. Many authors8,4,3
had reported that ultrasound and MRI can reliably establish the
diagnosis of cysticercosis. Out of the six cases reported by
Jhankaria et al3, five had clear cysts that displayed
low signal intensity on T1-weighted images and high signal
intensity on T2-weighted images. Four of these cysts had
scolices within them. One patient had an ill-defined
hyperintense lesion on T2-weighted images without any clear
cyst. Similar to their observation, perilesional edema was
remarkable in the image findings of present case. On the basis
of MRI finding we had started the antihelmenthic treatment (albendazole)
and the child responded well. The introduction of praziquantel
and albendazole made the treatment of cysticercosis more
promising. Multi-center clinical trials found that albendazole
is superior to praziquantel. Recent clinical trials have reduced
the duration of treatment with albendazole to 8 days1.
However we treated the child as per the old régime with 4 weeks
of albendazole therapy. For initial one week we had combined an
anti-inflammatory drug for the inflammation to subside. To
conclude, cysticercosis should be kept as a differential
diagnosis for any focal myositis even with out any neurological
abnormalities.
Reference :
-
Vanijanonta
S. Cysticercosis by the Year 2000: an Update. The J tropical med
parasit 1999; 22 (1): 34-40
-
Vorachai S,
Suphaneewan J. An Intramuscular Cysticercosis, A Case Report
with Correlation of Magnetic Resonance Imaging and
Histopathology. Chot Mai Het Thang Phaet
2007; 90(6): 1248-1252
-
Jankharia
BG, Chavhan GB, Krishnan P et al. MRI and ultrasound in solitary
muscular and soft tissue cysticercosis. Skeletal Radiol 2005;
34: 722726
-
Asrani A,
Morani A. Primary Sonographic Diagnosis of Disseminated Muscular
Cysticercosis. J Ultrasound Med 2004; 23:1245-1248
-
Khan RA,
Chana RS. A Rare Cause of Solitary Abdominal Wall Lesion. Iran J
paediatr 2008; 18(3): 291-292
-
Ogilvie CM,
Kasten P, Rovinsky D et al. Cysticercosis of the triceps: an
unusual pseudotumor. Clin Orthop 2001; 382: 217221
-
Gutierrez
Y. Cysticercosis, Coenurosis, Sparganosis and Proliferating
Cestode Larva. In: Diagnostic pathology of parasitic infections
with clinical correlations, 2nd ed. Oxford University Press US
2000. p. 636-638
-
Mani NB,
Kalra N, Jain M et al. Sonographic diagnosis of a solitary
intramuscular cysticercal cyst. J Clin Ultrasound 2001; 29:
472475.
-
Bilge EF,
Baris T, Ulku K et al. Solitary Cysticercosis in the
Intermuscular Area of the Thigh: A Rare and Unusual Pseudotumor
with Characteristic Imaging Findings [Case Report:
Musculoskeletal Imaging]. Journal of Computer Assisted
Tomography 2005; 29(2): 260-263
-
Abdelwahab
IF, Klein MJ, Hermann G et al. Solitary cysticercosis of the
biceps brachii in a vegetarian: a rare and unusual pseudotumor.
Skeletal Radiol 2003; 32: 424-428
-
Brown ST,
Brown AE, Flipa DA et al. Extraneural cysticercosis presenting
as a tumour in a seronegative patient. Clin inf dis1992;
14:53-558.
-
Falco OB,
Pleweig G, Wolf HH et al. Diseases caused by worms. In:
Dermatology, Falco OB, Plewig G, Wolff HH, Winkelmann RK Eds.
3rd ed. Berlin, Springer-Verlag; 1984. p. 262-274), Pp:291-292
|

