|
Eran Maman*,**, Guy
Morag*,**, Oleg Safir*, Mony Benifla*, Gavriel Mozes**, Erin
Boynton*
*
Department of Orthopedics, Mt. Sinai Hospital, 600 University Avenue,
Suite 476D, Toronto, Ontario, Canada M5G 1X5
**Department of Orthopedics B,
Tel-Aviv Sourasky Medical Center and the Sackler Faculty of
Medicine, Tel-Aviv University, Tel-Aviv, Israel
Address for Correspondence:
Eran Maman, MD,
Department of Orthopedics B,
Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel 62439.
Telephone: 97236973920, Fax: 9723694546
E-mail: eemaman@gmail.com
|
|
Abstract:
Background: Injury to the axillary nerve has devastating
results. Variations in the distance between the acromial edge
and axillary nerve range from 20-70 mm. The purpose of this
study was to anatomically analyze the relations between the
anterior trunk of the axillary nerve and the acromion in order
to provide guidelines for minimizing intraoperative iatrogenic
neural injury.
Methods: The distances between the axillary nerve and the
posterolateral, midlateral , and anterolateral edges of the
acromion were measured in 60 cadaveric shoulders (30
fresh cadavers). The correlations between these
measurements to the weight, height and sex of the cadavers were
statistically analyzed.
Results: The distances between the axillary nerve and all
three acromial anatomic landmarks significantly correlated with
the cadavers height (p<0.001) The axillary nerve was found as
close as 30-35 mm distal to the acromion in cadavers shorter
than 170 cm, (5.7), whereas the minimal distance between the
acromion and axillary nerve was 45-49 mm in cadavers taller than
170 cm.
Interpretation: We
recommend using the height of the patients as an index for
determining the relations between the axillary nerve and the
acromion. We defined a general safety zone for patients shorter
and those taller than 170 cm. We believe that using these
guidelines can minimize iatrogenic injuries to the axillary
nerve better than the commonly used 5‑cm safety zone when
performing a deltoid split.
This study quantifies the relative risk of injury to the
axillary nerve during shoulder surgery based on the patients
height and provides guidelines in avoiding such injury
J.Orthopaedics 2008;5(2)e7
Introduction:
Iatrogenic nerve injury is one of the most dreaded complications
of any surgery, and on potential site is axillarys nerve injury
associated with deltoid muscle surgery, be it arthroscopic or
open. Injury to the anterior trunk of the axillary nerve leads
to devastating loss of shoulder flexion strength. 1.
The exact location of the nerve varies, and few cadaveric
studies have examined the variability of the axillary nerve and
its course in the deltoid muscle. 2,3,4,5,6,7,8,9
The axillary nerve has been described as being located about 5-7
cm vertically from the lateral edge of the acromion, and even
less as the nerve curves upwards. 2,10,11,12,13 Some studies
demonstrated that the distance from the lateral edge of the
acromion to the axillary nerve (A-A distance) might be as much
as 2-3.1 cm shorter 2,7. These conflicting data complicate the
estimation of a safety zone for incisions around the deltoid
muscle.
There have been several attempts to correlate the axillary
nerves location to the patients surface anatomy. A study by
Vathana et al. showed that the length of the acromion was not
useful nor did the length of the arm correlate with the distance
of the axillary nerve from the acromion, the latter finding in
disagreement with an earlier study by Burkhead et al. 3,7
However, a recent study by Cetik et al. demonstrated a
significant correlation between arm length and A-A distance.13
Several authors correlated the sex of the cadaver with the A-A
distance. 7,14 Others have tried to measure the distance from
the acromioclavicular joint and the proximal humerus to the
nerve. 6,14 Thus, the current guidelines for estimating the
location of the axillary nerve in different locations along the
deltoid muscle are either not clear cut or not easy to perform.
The Bone Bank, receives its organs (bones, tendons etc) from
relatively young donors that have been found to be suitable
tissue donors for re-implantation. The cretaria for tissue
donation includes no known pathology or previous surgery to the
donated site.
The team performing the harvesting procedure includes senior
orthopedic surgeons who have a special interest in shoulder
surgery. Having the rare opportunity to examine the anatomy of a
large amount of fresh cadaveric shoulders of relatively young
organ donors with complete medical history we conduct a study
that will provide guide lines for surgeons in shoulder surgery.
We hypothesized that there is a correlation between the height
of the patients and the distance of the axillary nerve from the
acromion. We suspected some positive correlation of this
distance to the patients body mass index (BMI) and sex as well.
Our purposes were to confirm the results of previous studies
regarding the axillary nerve location and course, and provide
reliable, practical surface anatomy guidelines in order to help
reduce iatrogenic injury to the nerve around the deltoid muscle.
To that end, we examined a group of fresh, relatively young,
cadavers of individuals who had not undergone any previous
relevant surgeries to the shoulder. These measurements were
later correlated to the patients selected physical attributes.
Material and Methods :
After obtaining the Institutional Review Board
approval, 62 fresh shoulders from 31 cadavers were traced for
our study. 2 shoulders were not suitable (one sustained a
fracture to the proximal humerus and the other was status post a
previous surgery). The remained 60 shoulders (mean age 45.37
years, median 50.5 range 15-74, 17 males) had no previous known
pathology or surgery.
Dissection was performed while observing several rules to
minimize the chances of bias and to unify the results: the
deltoid muscle was always attached to the bone on both sides and
it was reflected backward only to the point of measurement (i.e.
moving the point of reference of the nerve with the acromion and
humerus). The measurements were done with the arm in about 30º
abduction and in neutral rotation.
On dissection the skin was removed until full exposure of the
entire anterolateral deltoid muscle was achieved, followed by
delto-pectoral splitting. The anterior deltoid was sharply
released from its origin at the acromion while retracting the
muscle laterally and posteriorly. When reaching to the
anterolateral tip of the acromion The distance from the inferior
anterolateral tip vertically to the superior border of the
anterior branch of the axillary nerve was measured (Figure 1)
with a plastic ruler commonly available in the operating theatre
(Securline, Surgical Skin Marker, San Fernando, CA). further
release of the deltoid posteriorly was done until the middle
acromion was exposed and the same on the other end of the muscle
on the humeral attachment. A second measurement was taken from
the inferior edge of the mid lateral acromion vertically to the
axillary nerve. (Figure 2) Completing the deltoid release until
the posterolateral acromion and the posterior attachment to the
humerus, a third measurement was taken from the posterolateral
corner of the acromion vertically to the axillary nerve. (Figure
3)
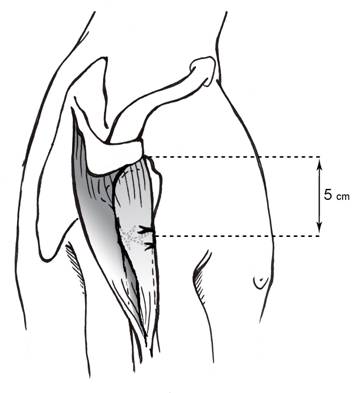
Figure 1: Axillary nerve
measurement from the inferior anterolateral tip of the acromion
vertically to the superior border of
the anterior branch of the
nerve
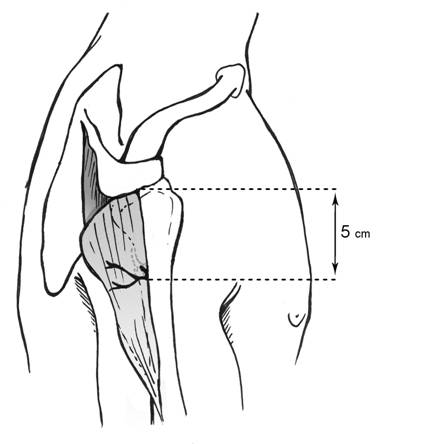
Figure 2: Axillary nerve
measurement from the inferior edge of the mid‑lateral acromion
vertically to the anterior branch of the nerve
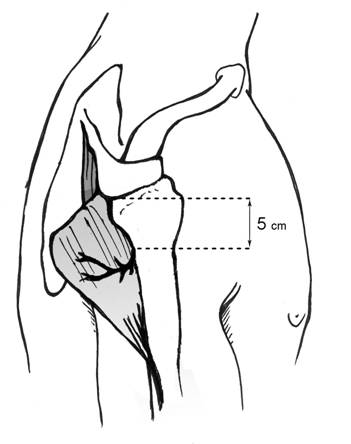
Figure 3: Axillary
nerve measurement from the inferior anterolateral tip of the
acromion vertically to the superior
border of the nerve
Three senior orthopaedic surgeons were involved in the
dissections and measurements (E.M, G.M., O.S.)
We correlated these measurements with the age, sex, side (right
or left shoulder), height, weight (which we obtained from the
medical records) and BMI (weight/height2).
Statistical analyses of
height, weight and BMI were done by univariate logistic
regression analysis, with the dependent variable being average
A‑A distance of greater or less than 5 cm. The distance of 5 cm
served as a point of comparison since it was the median distance
of our study population. The level of statistical significance
was set at p<0.05. The cadavers were divided between the ones
that were ≤170 cm tall and those that were >170 cm tall, and
Pearson's chi-square and
Fisher's Exact Tests were used
with confidence interval (CI) OF 95% for comparisons between the
two groups.
Results :
The vertical A-A distance at three measurement sites of the same
cadaver were no different between the right and the left
shoulders (p=0.59). The median A-A distance was 50 mm, the mean
distance was 50.3 mm and the range was
30.070.0 mm. The distance was <40 mm in only four
shoulders of two cadavers (164 and 170 cm tall) for which the
respective measurements were 35-38 mm in the posterior tip of
acromion and mid‑acromion and 30-33 mm in relation to the
anterolateral tip of the acromion.
The A-A distance differed
according to the location of the measurements. The mean A-A
distance for the three points of measurements (the posterior
tip, the mid‑acromion and the anterolateral tip) was 51.7, 50.8,
and 48.5 mm, respectively (Table 1). There was a significant
difference between the anterolateral measurements and those of
the two others sites (p<0.001), but there was no significant
difference between the measurements at the midlateral and the
posterior sites.
Table 1. The
vertical distance of the axillary nerve from the inferior
acromion at three measurement sites.
|
Vertical distance (acromion-axillary
n.) in mm |
|
Heights cm |
anterior (mean) |
anterior (range) |
middle (mean) |
middle (range) |
posterior (mean) |
posterior (range) |
|
≤170 (n=28) |
44.0 |
30-52 |
46.6 |
35-55 |
47.2 |
35-55 |
|
>170 (n=32) |
52.3 |
45-60 |
54.5 |
45-68 |
55.6 |
49-70 |
Discussion :
Although the popularity of arthroscopic procedures is rising,
the role of open or mini open procedures around the shoulder is
still major. Procedures such as reverse total shoulder
prosthesis, mini open rotator cuff repair, resurfacing
arthroplasty or fracture fixation are commonly performed through
a deltoid split.. in these procedures shoulder surgeons need to
estimate the location of the axillary nerve in order to avoid
iatrogenic injury. Anatomical variations are relevant whether
the procedures are arthroscopic or open. Guidelines for
estimating the location of the axillary nerve in different
individuals will lower the risk for iatrogenic injury during
these procedures.
The course of the axillary nerve runs along the deep surface of
the deltoid muscle and is parallel to the acromion. It curves
upward closer to the acromion as it progress anteriorly. The
nerve is commonly described as being located 5-7 cm distal to
the acromion, but it might be as close as 2-3.1 cm.
10,11,12,5,13,2,7 Past measurements were carried out using
various anatomical landmarks. Bono et al. described the distance
of the axillary nerve in relation to the proximal humerus and
found it to be an average of 6.1 cm.6 Brayan et al. measured the
distance starting from a 5 cm vertical incision (deltoid split)
to the axillary nerve: the average A A distance was 5.9 cm for a
posterior incision and 5.65 cm for an anterolateral incision.
More disturbing was the fact that the deltoid split actually
crossed the axillary nerve in 7 anterior and 4 anterolateral
incisions.5
According to Kamineni et al.s measurements, the average
distance of the axillary nerve was 5.7 cm (range 3.57.0 cm) in
relation to the tip of the acromial process along the lateral
aspect of the arm, and 5.1 cm (range 3.58.5 cm) along the
anterior aspect.12 Thus, while the literature can provide
reliable information on surface anatomy, variations such as
these in describing the course of the nerve emphasize the need
for reliable guidelines for conducting surgery at this site.
Vathana et al. 3 attempted to correlate locations of the
axillary nerve and patients relevant physical data, such as the
length of the arm and of the acromion, and Burkhead et al.
suggested guidelines to help predict the location of the
axillary nerve. The latter authors found a gender based
difference in the distance from the acromion to the nerve as
well as in the length of the arm. They concluded a deltoid split
of no more than 2.5-3.75 cm from the acromion is safe for males
and 2.5 cm for females, and that shorter deltoid splitting is
safe when the arm is abducted. 3,7 Recently the correlation of
the distance from the acromion to the nerve and the length of
the arm has been further established by Cetik et al. they found
a significant correlation between arm length and both anterior
and posterior distances.13
Nassar et al. 14 proposed an axillary nerve index based on the
distance of the nerve from the acromioclavicular joint to the
length of the deltoid. This calculation requires the drawing of
a line from the anterior border of the clavicle and acromion
laterally over the deltoid, locating the deltoid tuberosity, and
multiplying the derived value by 0.48 for males and 0.41 for
females. The result of this equation is an estimation of the
distance of the axillary nerve from the acromioclavicular joint.
Although accurate, this method requires identifying the deltoid
tuberosity, which may sometimes be difficult (e.g., obesity,
edema, and change in arm length post trauma). Moreover, this
index refers to incisions planned along this line only and might
not be accurate for more posterior ones.14
We sought to provide guidelines that would be practical, user
friendly and reliable while, at the same time, not limiting the
surgeon to a too narrow safety zone. We tried to provide
uniformity in the measurements and have them reflect operating
conditions as much as possible (e.g., the arm in adduction or no
more than 30 degrees of abduction and natural rotation). Another
confounding factor, contracture of the muscle after detachment
from the bone, was avoided by measuring the distance when the
muscle was still attached to the bone on its ends. Finally, we
bore in mind that positioning the arm in abduction or rotation
and previous trauma to the arm may change the length of the
muscle/bone and that these factors will affect the measurements.
Our data support the findings of previous anatomical
investigations on the distance of the axillary nerve from the
acromion that show a great variety in the A-A distance (30-70
mm). 10,11,12,5,2,7,13. In 60 shoulders of the 30 cadavers we
studied (51.7%), the distance was <50 mm from the anterolateral
corner of the acromion, <50 mm in 14/60 (23.3%) from the
midlateral acromion and <50 mm in 11/60 (18.3%) from the
posterolateral acromion. In only 4 shoulders (6.66%) was the
distance <40 mm.
The A-A distance shortens as we move anteriorly. We demonstrated
a significantly shorter distance on the more anterior
measurements compared to the others measurements (p<0.001), a
finding that can be explained by the nerve curving upward, by
the fact that our measurements were done from the inferior edge
of the acromion where it curves downward (type II/III) or has
anterior osteophytes, or both.
The A-A distance changed significantly with height (p<0.001).
The ≤170 cm cadavers had an A-A distance ranging between 30-55
mm while the ones taller than 170 cm had a range of 45-70 mm. In
order to find the safety zone (calculated from the
inferolateral acromial edge to the axillary nerve) in which the
chances for iatrogenic injury to the axillary nerve will be far
less likely; we examined the smallest measurements for each
group. The safety zone can be as small as 30 mm anteriorly or 35
mm mid laterally and posteriorly in the shorter group, while the
axillary nerve can be expected to be as close as 45 49 mm in the
taller group. We further subdivided the taller cadavers into one
group 171-180 cm in height and another group >180 cm in height
and found no significance difference between them.
Unlike others who showed gender differences as being
significant, the A-A distance between our female and male
cadavers was of borderline significance(p=0.063). Thus, the two
factors of height and location defined the largest safety zone
at the posterolateral deltoid on an individual >170 cm and the
smallest safety zone on the anterolateral deltoid of shorter
ones.
The small number of shoulders is a limitation of our study.
Greater numbers of shoulders from different cadavers might have
allowed us to arrive at more precise guidelines. Although we
tried to avoid bias by applying strict rules in the way
dissection was carried as well positioning and taking
measurements, the fact that the measurements were taken by more
than one surgeon might create interoberver bias. All
measurements were taken from the undersurface of the acromion,
which contributes to shorter and safer measured distances;
however, they do not faithfully reproduce the surgeons
measurement from the top aspect of the acromion intraoperatively.
Conclusion:
The novelty of our study is by providing new and applicable
guidelines for avoiding axillary nerve injury during shoulder
surgery. According to the results of the present study, the
common expectation of the axillary nerve being located around 50
mm from the lateral edge of the acromion will be correct in
about half of the cases. There is a significant correlation
between the patients height and the vertical distance measured
in all examined sites. The shorter the patient and the more
anterior the deltoid incision, the shorter will be the distance
of the axillary nerve to the acromion.
Guidelines:
-
Height ≤170 cm (5.7): the safety zone
might be as short as 30 mm anteriorly or 35 mm midlateral and
posterior.
-
Height >170 cm (5.7): the axillary nerve
can be expected to be as close as 45 mm vertically from the
anterolateral acromion and 49 mm from mid‑lateral and
posterolateral acromion. In some of these patients the nerve
may lie as far as 70 mm from the inferior acromion. (Our
measurements were in relation to the inferior acromion: since
they will be taken from the superior edge intraoperatively,
the surgeon can add the width of the acromion to the safety
zone.)
Reference :
-
Perlmutter GS. Axillary nerve injury.
Clin.Orthop.Relat Res. 1999; 28-36.
-
Kontakis GM. Steriopoulos K. Damilakis J.
Michalodimitrakis E. The position of the axillary nerve in the
deltoid muscle. A cadaveric study. Acta Orthop.Scand.
1999; 70: 9-11.
-
Vathana P. Chiarapattanakom P. Ratanalaka R. Vorasatit
P. The relationship of the axillary nerve and the acromion.
J.Med.Assoc.Thai. 1998; 81: 953-57.
-
Kulkarni RR. Nandedkar AN. Mysorekar VR. Position of
the axillary nerve in the deltoid muscle. Anat.Rec. 1992;
232: 316-17.
-
Bryan WJ. Schauder K. Tullos HS. The axillary nerve
and its relationship to common sports medicine shoulder
procedures. Am.J.Sports Med. 1986; 14: 113-16.
-
Bono CM. Grossman MG. Hochwald N. Tornetta P, III.
Radial and axillary nerves. Anatomic considerations for humeral
fixation. Clin.Orthop.Relat Res. 2000; 259-64.
-
Burkhead w z. Schienberg R R. Box G. Surgical anatomy
of the axillary nerve. J shoulder elbow surg. 1992;
31-36.
-
Uno A. Bain GI. Mehta JA. Arthroscopic relationship
of the axillary nerve to the shoulder joint capsule: an anatomic
study. J.Shoulder.Elbow.Surg. 1999; 8: 226-30.
-
Loomer R. Graham B. Anatomy of the axillary nerve and
its relation to inferior capsular shift. Clin.Orthop.Relat
Res. 1989; 100-5.
-
Hoppenfeld S, De Boer p, eds. Surgical exposures in
orthopaedics.J.B. Lippincott company, Philadelphia, 1994.
-
Hollinshead W H, ed. Anatomy for surgeons.Harper
and Row, New York, 1969.
-
Kamineni S. Ankem H. Sanghavi S. Anatomical
considerations for percutaneous proximal humeral fracture
fixation. Injury 2004; 35: 1133-6.
-
Cetik O. Uslu M. Acar HI. Comert A. Tekdemir I. Cift
H. Is there a safe area for the axillary nerve in the deltoid
muscle? A cadaveric study. J.Bone Joint Surg.Am. 2006;
88: 2395-9.
-
Nassar JA. Wirth MA. Burkhart SS. Schenck RC, Jr.
Morphology of the axillary nerve in an anteroinferior shoulder
arthroscopy portal. Arthroscopy 1997; 13: 600-05.
|

