|
Abstract:
Improvements in
spinal instrumentation system has been the rule of current practice, recently interspinous
spacers has been used to treat lumbar disc disease. This sytem
relies on the principle of distraction in the interspinous area
with indirect decompression of the roots by enlarging the
intervertebral neural foramen.
We
studied the results of a similar principle but using a different
system. We analyzed
the role of biologic distraction and global fusion, with
maintenance of the disc space using Modified Quasi-Claw
technique, in lumbar spine for the treatment of chronic lumbar
disc pathology. The modified Quasi-Claw makes use of a
distraction claw with supralaminar hooks below and infralaminar
hooks above with biologic distraction applied between them. We
conducted a prospective study in a series comprising 70 patients
(142 segments) with lumbar disc pathology with an average follow
up of 2.5yrs. Average preoperative Oswestry disability index was
74.22 and Visual analogue scale(VAS) score was 68.12. Biological
distraction was achieved using the principle of Modified
Quasi-claw and fusion achieved using posterior lumbar interbody
fusion (PLIF) with minced iliac crest graft along with
posterolateral fusion (global fusion - 360˚ fusion).
Average post operative Oswestry disability index was 26.64 and
VAS score was 14.32 respectively which was found to be
statistically significant (p<0.01 ). Biological distraction
restores disc height, helps in root canal decompression by
increasing the size of intervertebral foramen, improves the load
bearing ability of anterior ligaments and muscles and helps in
maintaining the spinal balance. It also stabilizes the spine by
avoiding the abnormal intrinsic instability between the motion
segments. The authors consider that biological distraction using
the principle of Modified Quasi-Claw with PLIF and
posterolateral fusion in the treatment of chronic lumbar disc
pathology is a novel concept with a good outcome.
J.Orthopaedics 2008;5(1)e12
Keywords:
Biologic distraction; Modified Quasi Claw; Posterior lumbar
interbody fusion (PLIF); Lumbar segmental instability;
functional spinal unit.
Introduction:
The management of
chronic disabling low back pain due to lumbar disc disease has
always been a controversy in modern orthopedics. Several treatment methods have been described but none of
them have given satisfactory results. Hence there has always been a quest for newer techniques
in this field. We
describe a new technique with good and reproducible outcome in
the treatment of Lumbar disc disease.
Crock H V1
described internal disc disruption. The abnormality in the
internal architecture of the disc could cause mechanical back
pain and referred pain. The outer third of the annulus of the
intervertebral disc has nociceptive capability and this could
account for discogenic back pain due to internal disc disruption 2, 3, 4.
Pedicular screws
used to achieve posterior lumbar interbody fusion (PLIF) has the
disadvantage that the graft should be locked in compression. The
compression further narrows the intervertebral neural foramen
and the patient may still be symptomatic. So distraction is more
biologic in the lumbar spine. The pedicular screw introduction
invariably needs radiologic imaging.
In this technique biologic distraction is applied to the
posterior complex which is more physiologic since the tension
surface of the spine is anterior complex when the spine is
considered as a single unit. The Quasi-claw does not need
imaging for introduction and is quick with minimum operating
time. This study attempts to delineate an easier and more
biologic method of
achieving PLIF with out imaging.
Several articles 5,6,7
describe treatments using anterior lumbar interbody fusion
(ALIF) and posterior
lumbar inter body fusion(PLIF) with instrumentation. Posterior lumbar interbody fusion (PLIF) 5,8,9
offers several advantages it restores disc height, maintains
root canal dimensions by increasing the size of the
intervertebral neural foramen. It also restores the load bearing ability of anterior
ligaments and muscles, helps in maintaining the spinal balance
and in maintaining lumbar lordosis. But with traditional method
of compressing the graft in the disc space there is an inherent
risk of narrowing of the disc space and the intervertebral
foramen especially when the graft collapses.
PLIF also helps in
stabilization of unstable functional spinal unit. The results of PLIF with instrumentation has been good.7,10,11,12,13,14.The
transverse diameter of neural foramen at the disc level of L5-S1
motion segment is around 7 mm. The diameter of the L5 root is around 7mm 15. This creates a critical area through which the root
escapes. Any reduction in disc height further reduces the
transverse diameter and results in compressive radiculopathy. So the only method to address this problem is by
maintaining the disc height and increasing the transverse
diameter of the intervertebral neural foramen to decompress the
root. This can be achieved by a constant biologic distraction
using Quasi-claw.
The currently
available segmental instrumentation and bone grafting have
helped in achieving posterior intertransverse and posterolateral
fusion with results comparable to that of PLIF 16, 17, 18. But these studies were done on patients with different
pathologies and different methods of treatment. Facetectomy was always a part of PLIF with the use of
tricortical grafts. But in this study no facetectomy was done,
and minced iliac crest graft were used instead of tricortical
iliac crest graft. The
disc space was maintained by posterior biological distraction
and instrumentation.
Quasi Claw
technique for spinal segmental stabilization is achieved by all
hook instrumentation. The supralaminar hook is inserted over the
inferior lamina and the infralaminar hook is inserted under the
superior lamina of the adjacent vertebra. This technique stabilizes a single motion segment. In modified Quasi Claw technique two motion segments are
stabilized instead of one. In
modified Quasi Claw technique supralaminar hook is inserted over
the inferior lamina and infralaminar hook is inserted under the superior lamina of the vertebra one level above the
adjacent vertebra.
Aim:
To determine the
effectiveness and evaluate the outcome of PLIF with biological
distraction and posterolateral fusion (global fusion) in the
treatment of lumbar disc disease using a different technique.
Material and Methods :
The study was
approved by the institutional ethics committee. Informed consent
was obtained from all the patients.
We
studied seventy cases of symptomatic Lumbar disc disease
operated between June 2000 and December 2005. All the selected
cases were in the age group of 30 to 73 years, irrespective of
the gender. Average age at the time of operation was 59 ±
7.6yrs. All the cases underwent PLIF with biological
distraction using posterior instrumentation and posterolateral
fusion. They were followed up for an average period of 2.5
years. A total of 142 segments were fused (Table1,). All the
cases were performed by the same senior surgeon (PGN).
Radiological
involvement of intervertebral disc were classified according to
Sarastes classification 19
Stage IA:
Normal
disc height without dehydration
Stage IB:
Normal
disc height with dehydration
Stage II: Disc
height decrease by less than 50%
Stage III: Disc
height decreased by at least 50%
Stage IV: Disc
height obliterated (with or without instability)
Potential risk
factors for achieving fusion like previous failed fusion, heavy
smokers (more than 1 packets of cigarette per day), heavy manual
laborers, fusion of more than two motion segments, instability, listhesis, excess weight
(more than 40 Kg in excess of predicted weight) were
specifically noted. Patient data about age, sex, walking
distance, working capacity, current employment, smoking,
VAS(visual analogue scale) and
Oswestry disability index were collected before and after
surgery.
Preoperative
investigations included plain X-rays, stress X-rays and MRI in
all patients. . Lumbar segmental instability was defined as a
motion greater than 4 degree of sagittal rotation or angulation
and translation of more than 4 mm 15
The inclusion
criteria for the patients were:
-
Patients with grade III and grade IV stages of Saraste19
of symptomatic lumbar disc disease in whom conservative
treatment has failed.
-
Only patients with
minimum two adjacent motion
segments are included.
-
Patients with grade I listhesis (degenerative).
-
Patients with symptoms of lumbar segmental instability
confirmed radiologically.
-
Previously operated symptomatic patients, who had undergone
spinal fusion, decompression and discectomy without
significant symptomatic relief.
-
Patients with
symptomatic psuedo-arthrosis, from previous un-instrumented
surgery.
Exclusion criteria
were,
-
Severe spinal canal stenosis.
-
Single level Disc disease irrespective of grade of disc
degeneration.
-
Infection.
-
Trauma.
-
Tumour.
-
Previously instrumented fusion.
The union was
probable when bony trabecular continuity was not clear, and
there was less than 4-degree mobility between adjacent fused
segments. Nonunion was defined as clear gap and motion greater
than 4 degree of sagital rotation or angulations and translation
of more than 4 mm 15.
But the presence of instruments will definitely hinder this
interpretation. The preoperative and postoperative disc height
was measured in all cases in lateral view midway between the
anterior and posterior longitudinal ligaments.
Patient data about
age, sex, walking distance, working capacity, current
employment, smoking, VAS and Oswestry disability index were
collected before and after surgery. Clinical improvements were
noted on the basis of improvement of back pain and working
capacity. Follow up was done at 3 months and there after at
regular intervals of 6 months
Clinical
improvements were noted on the basis of improvement of back pain
and working capacity. Follow up was done at 3 months and
thereafter at regular intervals of 6 months.
Out
of 142 segments fused, 100 segments had grade IV and remainder
had grade III degeneration. Disc involvement according to the
spinal levels is shown in Table2. 68 patients had adjacent one
level disc disease and two had three level disc disease. Single
level disc diseases were not selected.
Adjacent segments,
which were abnormal in the form of Grade III or IV disc disease,
were included in
the fusion mass to prevent post fusion symptoms. Four patients
had Grade IV disc degeneration with grade I listhesis, all were
at L4-L5.In all these patients reduction could be achieved with
the method described. Two patients were previously operated
cases for grade IV disc degeneration at L4-L5. Thirty two
patients had paraesthesia or sensory deficit. Radiculopathy was present in 10 patients in the form of
L5 or S1 root lesion. Tone and reflexes were normal. The average
follow up period was two and half years (between two to three
years). Out of 142
segments, 132 levels had clinico-radiological correlation. 10
segments (in the double level group) had atypical pain, which
had grade IV disc degeneration changes at adjacent segments and
so adjacent levels were included in the fusion mass. All
segments with grade IV degeneration had radiological signs of
Lumbar segmental instability (LSI).
Table 1. On
doing the Chi square test, a significant relationship (at 5%
level) was seen between grade IV disc degeneration and L5-S1
level.
|
|
L3-L4
|
L4-L5
|
L5-S1
|
Total
|
|
Grade
III
|
0
|
27
|
15
|
42
|
|
Grade
IV
|
2
|
36
|
62
|
100
|
Total
|
2
|
63
|
77
|
142
|
Table
2
<
Statistical
analysis:
Statistical analysis was performed by using Paired
t-test with using SPSS for Windows (version 12.0, SPSS,
Chicago
,
IL
). Comparisons between preoperative and postoperative disc
height,VAS, Oswestry score and
grade of degeneration and spinal level measurements were made
using the Paired t-test. The values were summarized as mean ±
standard deviation. A p value of < 0.05 was considered
significant.
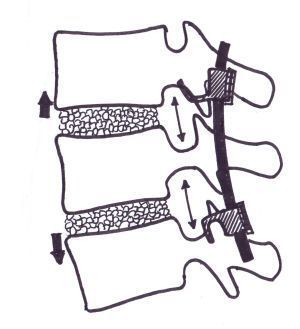
Fig.1
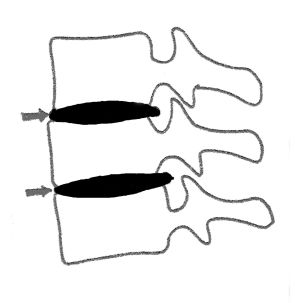
Fig.2
: Diagrammatic representation of biologic distraction
with maintenance of disc height and indirect decompression of
the nerve root by the enlargement of the intevertebral
neural foramen.
Surgical Technique:
Posterior lumbar
interbody fusion (PLIF) was done through a midline posterior
approach under general anaesthesia in the lateral decubitus
position. Laminectomy was performed, but facetectomy was not
done in any case. Discectomy
was done in all cases and end plates prepared till bleeding
subchondral bone was exposed. The nerve roots were retracted and protected. All hook
system was used in all the patients. Posterior instrumentation
with Modified Quasi Claw with short segment stabilization was
done using indigenously made supralaminar and infralaminar
claw.. The instrumentation consisted of supralaminar and
infralaminar narrow hooks, positioned in the superior and
inferior laminae after decompression.. The rods were contoured
to maintain the lumbar lordosis. Instead of tricortical iliac crest grafts, minced iliac
crest grafts were packed through the hole made for removal of
the disc. Disc height was maintained by biological distraction
and packing the disc space with bone grafts. Autologous iliac crest grafts were used in all patients. Maintenance of the disc space increased the size of the
intervertebral foramen and this indirectly decompresses the
nerve root (Fig1,2). Posterolateral fusion was done through
subperiosteal approach, and the bed of the graft, prepared by
subperiosteal dissection through the transverse process and
through the remaining lamina and spinous processes. Inter facetal fusion was achieved without facetectomy, by
exposing the subperiosteal region of superior and inferior
facets and bridging them with autologous iliac crest graft.
Radiologic assessment for integrity and placement on the
implants were done on the table before closure of the wound.
Postoperatively all patients were mobilized on the 3rd
day on a Knight Taylors brace. Postoperative stress x-rays where taken in all patients
after 8 weeks. The criteria for fusion was trabecular continuity8.All
the levels fused when there was less than 4 degree mobility as
measured by sagittal rotation angle or less than 4 mm
translation as measured as sagittal translation distance.
Results :
Mean VAS was
improved from 68.12 to 14.33 in this study. The range of VAS was
15-80 preoperatively , while post operatively it was 10-20. The
average reduction in VAS was 48.5 % (Table 3).
Average
preoperative Oswestry disability index was 74.22 and post
operatively was 26.64
(Table 4). The range was from 60-88 preoperative and 20-36 post
operative so the reduction in disability was 49%. Since the
intervention involved a single variable with paired measurements
in each subject the paired students t
test was used as the test of statistical significance. This was
statistically significant with the p-value <0.01 .So there
was significant statistical improvement in Oswestry score
(p<0.05%). There was 4-fold increase in walking distance. Age
at the time of operation was 59 ± 7.6 yrs. The range being 30
to 73 yrs. The average operation time was 101.8 ± 50 mts and
the average blood loss was 633 ± 25.4 gms.
Excellent
correction of disc height could be achieved post-operatively
(Fig3,4). Average preoperative disc height was 4.72 ± 1.49mm
and post operative was 9.81 ± 2.19mm with an average increase
of 5.12mm.(Table 5)

Fig.3:
Preoperative radiogram
showing Grade 1 lumbar spondylolisthesis at L4-L5 with unequal
and also reduced disc height at L4-L5.

Fig.
4: Post operative radiogram showing normal disc height and
parallel end plates with reduction of spondylolisthesis
Table
3
VAS Score (n=70)
|
|
Preoperative
|
Postoperative
|
|
Mean
|
68.12
|
14.33
|
|
Std.
Deviation
|
9.89
|
2.49
|
p value <
0.01
Table 4
Oswestry Score(n=70)
|
|
Preoperative
|
Postoperative
|
|
Mean
|
74.22
|
26.64
|
p value <
0.01
Table 5
Disc Height (n=142)
|
|
Preoperative(mm)
|
Postoperative(mm)
|
|
Mean
|
4.72 ± 1.49mm
|
9.81 ± 2.19mm
|
Twelve patients
were symptomatic even after surgery. Of these twelve, eight
patients had low back pain, 4 patients had leg pain at latest
follow up. Out of these 12 patients,10 patients said their
symptoms improved after surgery, but 2 patients had same
symptoms even after surgery.
None of the
patients had nonunion. 4 patients had doubtful interbody fusion
but had demonstrable posterolateral union and the sagital
translation less than 4mm, sagital angulation less 4 degree. 32
patients returned to their original duties. Twenty two patients
returned to light duties after surgery. There was an improvement
of 77% in working ability according to Oswestry scale.
Four
patients developed urinary tract infection, treated successfully
with antibiotics. Two patients had delayed wound healing and
persistent iliac crest pain for six months, both were known
diabetic patients. Two cases had paralytic ileus, which
responded to treatment.
Discussion :
It is always
desired that a comprehensive approach is a must in the
management of chronic disc disease with low backache (LBA). But
the complexity of the problem puts the treating surgeon in a difficult situation. Morgan FP et
al 20 drew attention to the association between
annular tears, radiographic instability and LBA and the use of
flexion extension views in diagnosing
lumbar segmental instability. Kirkady Willis21 et al defined stages of instability and focused on
anteroposterior and lateral bending radiographs in chronic
lumbar disc disease. They described three stages of disc
degeneration.
-
Stage I: circumferential and radial tears in the disc
annulus and localized synovitis with hypermobility of facet
joints.
-
Stage II: characterized
by internal disruption of disc, progressive disc resorption,
degeneration of facet joints with capsular laxity,
subluxation and joint erosion leading to instability.
-
Stage III : marked by osteophytosis and spinal stenosis,
where the body tries for stabilization.
Frymoyer
JW22 et
al defined the basis of mechanical instability in chronic lumbar
disc disease and described
that the disc degeneration can result due to aging.
Leufven 23
et al reported 93% fusion and 73 % satisfactory outcome using
circumferential fusion and 62% patients had returned to original
work. Some other authors 5,6,7,8,10 have reported 70%
satisfactory outcome when PLIF was combined with posterolateral
fusion and instrumentation. Degenerative lumbar segmental
instability is a concern for spinal surgeons even today.
Accurate pre operative identification of each component of the
problem, which produces a particular symptom, should be
addressed individually for the complete relief. PLIF is commonly
advocated as a method of treating mechanical low back pain
including LSI (Lumbar Segmental instability) with 70-80 % fusion
rate and patient satisfaction are reported in literature 1,5,24 and 75 90% return to work is also reported. Accelerated degeneration of the adjacent segments was
described in literature.25,26,27,28 Once a particular
functional spinal unit is fused, more stress occurs at the
adjacent spinal unit, accelerating degeneration and Lumbar
Segmental Instability.27 Instability in a particular
functional spinal unit starts as sclerosis of the end plates
with disk space narrowing, (Figure 1).
It
causes hypertrophy of the ligamentum flavum and posterior longitudinal ligament. Later on
there is translation listhesis and angulations that indirectly narrows the intervertebral foramen and
compresses the root. This will result in spinal canal stenosis,
facet joint arthritis, capsular ligament laxity of the facet
joint with facetal instability resulting in facet induced pain
and discogenic pain. It
can also lead to claudication and neurological deficit (Table 1)
from global spinal instability in a particular functional spinal
unit.It is the surgeons duty to intervene at any of these
stages to reverse this cascade of processes, so that the
symptoms can be reversed. Instability should be addressed by
instrumentation, which later on should be taken over by interbody and posterolateral fusion . Otherwise, the
implant will fail in the long run. Canal compromise should be
addressed by decompression.In this study, stress is given to
maintain the disk height by the technique of jacking up the disk
space so that this will indirectly increase the size of the
intervertebral foramen and decompressing the root, thus
relieving the radiculopathy. Adjacent functional spinal units
are usually abnormal and should be included in the fusion mass
to avoid re operation for LSI at the adjacent functional spinal
unit.The etiology of low backache is often multifactorial, including organic and nonorganic causes.
This study was not intended to address all of the manifestations
of low back pain, but it was directed at evaluating the efficacy
and safety of the technique of fusion and instrumentations.
Chronic low backache cause prolonged disability, anxiety and
discomfort. It is often difficult to treat such patients because
of difficulties in diagnosis and interpretations of
investigations. There is also an important factor of
psychosomatic elements. Clinicoradiological correlation revealed
high intensity zone in MRI, loss of disc height, end plate
changes and grade one listhesis, which were addressed during
treatment14. Fusion rate was 100%. The assessment was
prospective. The work ability out come was good probably because
of better restoration of disc height, maintenance of lumbar
lordosis and better load distribution through the spine.
Nachemson et al 30 discussed the psychological
factors in this particular condition. In this study no attempt
was made to assess the psychological status of patients.
Psychological factors do affect pain, hence patient selection is
important. 83% patients had good outcome in this study. Usually
posterolateral fusion has been advocated for this condition to
avoid morbidity associated with PLIF.17. In this
study 100% fusion rate could be achieved by disc excision and
instrumented PLIF and posterolateral fusion. This eliminates
chemical and mechanical sources of pain associated with internal
disc disruption. If the disc is not removed, it remains as a
source of continuous pain. Correction of instability and removal
of biological substances from degenerated disc eliminates the
nociceptive stimulation of outer annulus 2,3,4
The motion segment
is a three joint structure with two facet joints and the
intervertebral disc 30. PLIF should be supported by
posterior instrumentation. PL fusion will enhance fusion at
PLIF. The current study shows 4 patients with doubtful PLIF, but
had good PL fusion.
This novel
technique has the advantage of extreme technical simplicity, it
does not need imaging for placement. In degenerative lumbar disc
disease, the traditional method of pedicular screw fixation
carries risk of implant failure due to osteoporosis and lack of
adequate screw purchase. The severity of osteoporosis is most
marked initially in the vertebral bodies. The posterior complex
is spared from osteoporosis. This technique makes use of
posterior complex for implant fixation which is more biomechanical stable. The traditional
method of pedicular screw involved compression using pedicular
screws .This will result in narrowing of intervertebral foramen and results in radicular pain.
This technique uses the technique of biologic distraction which
widens intervertebral foramen and reduces the chances of
radicular pains. If the lumbar spine is considered as a single
unit, the anterior complexes form the tension surface and the
posterior complex forms
the compression surface. Compression of the tension surface is
the well accepted method of stabilization of any bone. So
compression of the posterior complex with pedicular screws is
biomechanically incorrect. Biologic distraction of the posterior
complex indirectly leads to compression of the tension surface
i.e the anterior complexes and is more physiologic. Screw breakage is a known complication with the traditional
method but not a problem with this technique. The disadvantage
of this technique is that over distraction and lack of proper contouring of the rod leads to flat back
syndrome but adherence of the correct technique negates this
problem. Hook dislodgement could be a problem but correct
selection of hooks and their perfect placement avoids such
complication.
The traditional
method of pedicular screw fixation with compression to lock the
interbody graft has the disadvantage of narrowing the disc space
and intervertebral foramen especially when there is graft
collapse 31. The
primary concern of LSI is radicular pain and pain due to
instability. Radicular
pain can be addressed to a certain extent by foraminotomy but
the basic disease process is not corrected. So maintaining the disc height is of great importance
which can be achieved by biologic distraction and PLIF.
The transverse
diameter (from the ligamentum flavum to the vertebral body and
disc) of intervertebral foramen at L4 disc level is around 7mm.
Diameter of L4 root is around 7mm 15,31. So there is
a critical area through which root escapes 12,32.
Measuring the cross sectional area of the canal seems pointless
unless only the minimal area is considered 32 Narrowing of the intervertebral foramen will further
reduce this transverse diameter and result in radiculopathy.
Tandon etal 13
reported mean reduction in Oswestry disability index from 51
preoperative to 39-post operative so there is reduction of
disability by 12%. This series shows an improvement by 25%.
Biologic
distraction with instrumentation helps to maintain the disc
height resulting in prevention of compression of nerve roots in
the intervertebral foramen. By maintaining the disc space
transverse diameter can be increased and the root can be
indirectly decompressed. The
traditional 31 method of pedicular screws used to
compress the vertebrae together may reduce the disc height
especially when there is tricortical graft collapse. This will
lead to foraminal narrowing and radiculopathy resulting in
radicular pain even after solid fusion. The good outcome in this
study could also be either due to decompression of the roots or
dural sac, or could be due to short-term nature of this study.
The current study
shows that maintenance of disc height (Figure 2) and PLIF along
with posterolateral fusion had produced good clinical outcome.
More patients returned to their original work. PLIF improved the
dynamics of lumbar spine and restores lordosis, reduces
biochemical and mechanical factors of pain (Table 2). PLIF also restores the disc height, which is critical in
achieving good outcome. Thus stability achieved at the end of
fusion aids in good outcome. The facet joints and the annulus
fibrosus, which are the main stabilizers in the axial plane1,14
are only disturbed to the minimum.
Suk et al 33 reported
a mean pre-op disc height of
7.4 ± 5.6 mm which was improved to 9.8 ± 2.6mm. We obtained a
comparable result of average preoperative disc height as 4.72 ±
1.49mm and post operative as 9.81 ± 2.19mm with an average
increase of 5.12mm.
The global fusion
of 100% in this study does not correlate with the 80% recovery
by Oswestry (Table 3) probably due to the psychosomatic status
and multifactorial 30 nature of the particular
problem. Appropriate patient selection after psychosomatic
assessment could further improve the result. Posterior
distraction and instrumentation apply distraction to the
posterior lordotic (concave) side of the lumbar spine, which is
more physiologic than compression of the posterior aspect of the
lumbar spine. Since
the rods are contoured to the exact lumbar lordosis, there is
less chance of flat back syndrome. As long as the amount of distraction is just to maintain
the disc height and within physiological limits it does not seem
to affect the biomechanics of the spine. To the best of our
knowledge, there are no reported studies with use of such an
instrumentation technique to treat the particular group of
patients. But considering the short term nature of the study,
further studies with long term follow up are needed to have for
a more clear-cut analysis.
Conclusion:
The present
study has demonstrated that rigid instrumentation with biologic
distraction, using the principle of Modified Quasi claw; with a
short segment stabilization produces good clinical results in
the type of patients with chronic lumbar disc lesions as
detailed in this study. This is achieved by maintenance of disc
height, with indirect decompression of roots along with global
fusion. PLIF,
posterior instrumentation and posterolateral fusion (global
fusion) is effective in producing solid satisfactory fusion
rate. Good clinical
outcome is obtained is based on reduction in pain, return to
work or comparable activities. There was significant improvement
in Oswestry score (p < 0.01). The maintenance of disc height
is probably the single most important factor in improving
outcome in such patients.
Reference :
-
1. Crock HV. Observations on the management of failed spinal operations. J Bone Joint Surg Br.1976;58:193-9.
-
Kuslich SD, Ulstrom CL, Michael CJ. The tissue origin of low back pain and sciatica: a report of pain response to tissue stimulation during operations on the lumbar spine using local anesthesia. Orthop Clin North Am.1991;22:181-7.
-
Mooney V. Where is the lumbar pain coming from? Ann Med.1989;21:373-9.
-
Yoshizawa H, OBrien JP, Smith WT, Trumper M: The neuropathology of intervertebral disc removed for low back pain. J Pathol.1980;132:95-104.
-
Enker P, Steffee AD. Interbody fusion and instrumentation. Clin Orthop Relat Res. 1994;300:90-101.
-
Gertzbein SD, Betz R, Clements D, et al. Semirigid instrumentation in the management of lumbar spinal conditions combined with circumferential fusion. A multicenter study. Spine.1996;21:1918-25.
-
Tullberg T, Brandt B, Rydberg J, et al. Fusion rate after posterior lumbar interbody fusion with carbon fiber implant: 1-year follow-up of 51 patients. Eur Spine J.1996;5:178-82.
-
Brantigan JW, Steffee AD, Geiger JM . A carbon fiber implant to aid interbody lumbar fusion. Mechanical testing. Spine.1991;16:S277-82.
-
Zdeblick TA. A prospective, randomized study of lumbar fusion. Preliminary results. Spine.1993;18:983-91.
-
Brantigan JW, Steffee AD. A carbon fiber implant to aid interbody lumbar fusion. Two-year clinical results in the first 26 patients. Spine.1993;18:2106-7.
-
Franklin GM, Haug J, Heyer NJ, et al. Outcome of lumbar fusion in Washington State workers' compensation. Spine.1994;19:1897-903.
-
Lee CK, Vessa P, Lee JK Chronic disabling low back pain syndrome caused by internal disc derangements. The results of disc excision and posterior lumbar interbody fusion. Spine.1995;20:356-61.
-
Tandon V, Campbell F, Ross ER. Posterior lumbar interbody fusion. Association between disability and psychological disturbance in noncompensation patients. Spine. 1999;24:1833-8.
-
Vamvanij V, Fredrickson BE, Thorpe JM, et al. Surgical treatment of internal disc disruption: an outcome study of four fusion techniques. J Spinal Disord.1998;11:375-82.
-
Wesley W. Pake. Applied Anatomy of the spine. Chapter 2. The spine 4th edition volume 1 W B saunders company 1999 :43-44)
-
Lorenz M, Zindrick M, Schwaegler P, et al. A comparison of single-level fusions with and without hardware. Spine.1991;16:S455-8.
-
Wetzel FT, LaRocca H. The failed posterior lumbar interbody fusion. Spine.1991;16:839-45.
-
Leong JC, Chun SY, Grange WJ, et al. Long-term results of lumbar intervertebral disc prolapse. Spine.1983;8:793-9.
-
Saraste H, Brostrom LA, Aparisi T, et al. Radiographic measurement of the lumbar spine. A clinical and experimental study in man. Spine.1985;10:236-41.
-
Morgan FP,King T. Primary instability of lumbar vertebrae as common cause for low back pain. J Bone Joint Surg Br.1957;39:6
-
Kirkaldy-Willis WH, Hill RJ. A more precise diagnosis for low-back pain. Spine.1979;4:102-9
-
Frymoyer JW. Low back pain. The role of spine fusion. Neurosurg Clin
N Am.1991;2:933-54.
-
Leufven C, Nordwall A. Management of chronic disabling low back pain with 360 degrees fusion. Results from pain provocation test and concurrent posterior lumbar interbody fusion, posterolateral fusion, and pedicle screw instrumentation in patients with chronic disabling low back pain. Spine.1999;24:2042-5.
-
Agazzi S, Reverdin A, May D. Posterior lumbar interbody fusion with cages: an independent review of 71 cases. J Neurosurg.1999;91:186-92.
-
Brodsky AE. Post-laminectomy and post-fusion stenosis of the lumbar spine. Clin Orthop Relat Res.1976;115:130-9.
-
Lehmann TR, Spratt KF, Tozzi JE, et al.Long-term follow-up of lower lumbar fusion patients. Spine.1987;12:97-104.
-
Zucherman J, Hsu K, Picetti G 3rd, et al.Clinical efficacy of spinal instrumentation in lumbar degenerative disc disease. Spine.1992;17:834-7.
-
Whitecloud TS 3rd, Davis JM, Olive PM. Operative treatment of the degenerated segment adjacent to a lumbar fusion. Spine.1994;19:531-6.
-
Miyakoshi N, Abe E, Shimada Y, et al. Outcome of one-level posterior lumbar interbody fusion for spondylolisthesis and postoperative intervertebral disc degeneration adjacent to the fusion. Spine.2000;25:1837-42.
-
Nachemson A, Zdeblick TA, O'Brien JP. Lumbar disc disease with discogenic pain. What surgical treatment is most effective? Spine.1996; 21:1835-8.
-
Brantigan JW, Steffee AD, Lewis ML, et al. Lumbar interbody fusion using the Brantigan I/F cage for posterior lumbar interbody fusion and the variable pedicle screw placement system: two-year results from a Food and Drug Administration investigational device exemption clinical trial. Spine.2000;25:1437-46.
-
Farfan.H.F. Mechanical disorders of low back 1973 First Edition Lea and Friebger Philadelphia page:22-23
-
Suk SI, Lee CK, Kim WJ,et al. Adding posterior lumbar interbody fusion to pedicle screw fixation and posterolateral fusion after decompression in spondylolytic spondylolisthesis. Spine.1997;22:210-9.
|

