|
Abstract:
Background:Sonography
of the wrist has been suggested as a diagnostic tool in carpal
tunnel syndrome (CTS), but there are controversies with regard
to routine use of this tool in this disease. The aim of this
study was to determine the sonographic findings of severe CTS
with respect to carpal tunnel diameters, and to compare the
results with normal wrists.
Material & Methods:39
wrists of 21 patients with clinical and electro diagnosis (NCV)
evidence of CTS, who were candidate for surgery, and 42 normal
wrists underwent sonography using a 7.5 MHz linear probe. The
anteroposterior and transverse diameter of carpal tunnel, median
nerve, and cross section area of the nerve were evaluated and
compared.
Results:The
average anteroposterior diameter of carpal tunnel in CTS (8mm)
was less than normal wrists (10.05mm), which indicates a
narrower canal in the severe form of this disease.
Average diameters of median nerve were more
in CTS than normal wrists, with cross section area of 12.67mm2
and 10.29mm2 respectively.
Canclusion:
sonography is a useful modality in diagnosis of severe CTS. We
found out a decrease in anteroposterior diameter of carpal
tunnel in severe cases of this disease, a finding which has not
been considered previously. To evaluate the
US
results in mild to moderate CTS, more study will be needed
J.Orthopaedics 2007;4(4)e28
Keywords:
Carpal tunnel syndrome, Median nerve, wrist sonography, carpal
tunnel diameter.
Introduction:
Carpal tunnel syndrome (CTS) is caused by compression on the
median nerve at the wrist level and is the most common median
nerve pathology. CTS is more prevalent in females between 30 to
60 years old and is commonly presented with numbness, tingling
and pain in distal sensory distribution area of the median
nerve. Long-term nerve compression can cause thenar muscular
weakness and atrophy.
Generally any factor which decreases the carpal tunnel capacity
or increases the tunnel constitutes can initiate CTS symptoms
and signs (1, 2).
Diagnosis is based on history, physical examination
and also electro diagnosis evaluation of electromyography (EMG)
and nerve conduction velocity (NCV)] of the median nerve. (3)
These tests with sensitivity and specifity of 90% and 60%
respectively are still standard for diagnosis of CTS. Despite the
reliability of these tests, there are some patients in whom the
clinical findings and NCV, EMG results do not much with each
other. and (3, 4).
In recent years, sonographic examination of the median
nerve has been suggested as a useful diagnostic alternative to
EMG and NCV study.
Some authors believe the results of sonography are comparable
with NCV and it can be used as a primary diagnostic tool (5).
This study was performed to evaluate the sonographic
findings in severe carpal tunnel syndrome and normal subject,
and to compare the obtained results in two groups.
Material and Methods :
We conducted a prospective controlled clinical study during a
period of 19 months (between 2005 and 2006) in Imam Khomeini and
Razi hospitals. All of the patients with documented CTS referred
to our university orthopedic clinic were evaluated. The
diagnosis was based on clinical and electro-diagnostic
evaluations of EMG, NCV of median nerve.
Patients who were unresponsive to medical and supportive
treatments and were candidates for surgery entered the study.
Wrist sonography by an expert radiologist who was unaware from
study was performed for all patients, using a Hitachi EUB525
machine with a linear 7.5 MHZ transducer. 21 patients enrolled
the study, and treated by classic carpal tunnel release. 21 age
and sex matched healthy volunteers were chosen as controls and
sonography of
their carpal tunnel was performed for them too. Because
dimensions of carpal tunnel might be
different according to the size and body mass, and also most of
patients had bilateral CTS, so we tried to match the control
subjects with regard to sex , age and body weight with CTS
patients as could as possible. The measurements of diameters of
carpal tunnel, median nerve, and cross section of the nerve were
performed in two groups. Results were compared statistically
using Mann-whitney
and T- test.
Results :
21 patients (20 female and 1 male) with mean age of 48 years
(ranging from 29 to 63), and 21 healthy controls with the mean
age of 38 years (ranging from 24 to 58) entered the study...
Thirty nine wrists from case group with CTS, (the
operation was done on both hands in 18 female patients) and 42
wrists from control group were assessed by sonography
EMG, NCV of the median nerve in all of the patients was performed
as a routine for diagnosis... Mean duration of symptoms were 28
months, (6 months to 62 months).
The most common symptom was night paresthesia. Hand
pain was observed in 90 percent of cases. 71 percent of patients
reported pain accentuation at nights. (See table 2) Phalen test
was positive in 89 percent of patients and in 65 percent of
them, the test showed positive result in less than 30 seconds.
Tinnel test was positive in 97 percent, thenar weakness and
atrophy in 46 percent and nail dystrophic changes in 12 percent
of patients. Electro-diagnostic studies showed different degrees
of nerve impairment in all of patients. In 15 cases the symptoms
and signs were more severe in right hand (the dominant hand).
The results of wrist sonography in CTS group were as
follow:
The antero-posterior diameter of the median nerve in
the tunnel was ranged from 2 to 4 millimeter (mean and median
were 3.62 mm).
The transverse diameter was between 3-4 mm (mean
3.52). The carpal tunnel antero-posterior diameter at the
pysiform bone level ranged from 7 to 10 millimeter (mean were 8
mm) and its transverse diameter at the same level ranged from 17
to 21 millimeters (mean of 19.48 mm). Flexor retinaculum
thickening and reduced echogenisity of the median nerve were
observed in 8 cases this finding was not seen in normal wrists.
In one case the median nerve bifurcation was seen. (Table 1, 2)
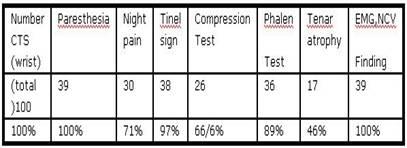
Table
1: Results of clinical and electro diagnostic findings in
CTS group
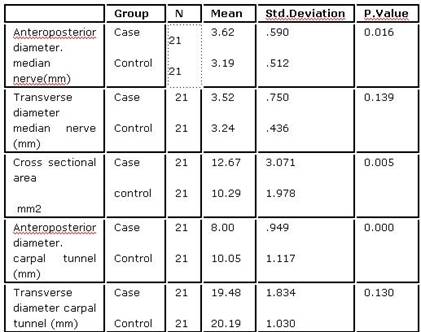
Table 2: Results of sonographic findings in CTS
and control group
Results of sonographic study in control group were as
follow:
The antero-posterior diameter of the median nerve at
the tunnel was ranged from 3 to 4 millimeter (mean and median
were 3.19 mm). Transverse diameter of the median nerve was 2-4
millimeter (mean of 3.24 mm). The antero-posterior diameter of
carpal tunnel at the pysiform bone level ranged from 7 to 11
millimeter (mean and median were 10.05 mm) and its transverse
diameter at the same level ranged from 19 to 22 millimeters
(mean of 20.19 mm).(Table 3 and 4)
Discussion :
The few papers published on the use of sonography in carpal
tunnel syndrome suggest it as
a useful diagnostic tool..
The main findings in favor of CTS has been increase .in
cross-sectional area of median nerve with an area larger than
10.3 mm2 being highly predictive of carpal tunnel
syndrome.(6) In symptomatic CTS with severe EMG and NCV
abnormalities, the median nerve cross- sectional area is almost
always more than 11 mm2.(7) In these conditions, the
median nerve swelling is observed at its entry to the tunnel and
seems wide in that area. (8). Fig: 1

Fig 1:
Swelling of the median nerve at entry of carpal tunnel
El Miedany et al compared the sonographic
findings of CTS patients with normal subjects and found out increase
of the median nerve cross sectional area to more than 10 mm2
is highly compatible with clinical and NCV findings in CTS
patients. They concluded that ultrasonography is a new and
valuable tool in diagnosis and follow up of this disease. (9)
Yesildag et al measured the median nerve cross sectional
area at three points (before, through and after the transverse
retinaculum). The mean value of three mentioned measurements had
88 percent sensitivity and 94 percent specificity in diagnosis
of CTS. (10)
Serria et al studied 40 hands of CTS patients and
compared the results with 24 normal controls. The most reliable
finding in sonography was increased flexor retinaculum thickness
and cross sectional area of the median nerve with a specificity
of 60 percent for CTS diagnosis. (7)
Ultrasonography is a noninvasive cost
effective diagnostic tool that takes much less time than NCV
without unpleasant sense of electrode usage in NCV and EMG for
patients. It is especially useful in diagnosis of some carpal
tunnel causes such as abscess and space occupying lesions.
Assessment of the flexor tendon movements and post operative
follow up of patients are some of other advantages of wrist
sonography. (8, 11)
Sonography can also be used to estimate
the wrist angle in which the least pressure is transferred to
the median nerve, guiding the steroid injection to inflamed
flexor digitorum tendon sheaths, guiding the release of carpal
tunnel, assessing the existence of nerve swelling before canal
and also the nerve widening through the canal, and thickening
and palmar bowing of the carpal retinaculum. (8, 11, 12, 13)
Because all of patients in our study were of severe CTS, so the
sonographic findings do not correlate in mild or moderate forms
of disease.
The results of our study shows a meaningful statistical
difference between two groups with regard to AP diameter of
median nerve, cross sectional area of it, and AP diameter of
carpal tunnel, with P.value < 0.005. However the difference
between transverse diameters of tunnel was not significant in
two groups. The average cross sectional area of median nerve in
CTS and control group were 12.67 mm2 and 10.29 mm2 respectively.
The range of these values in CTS and normal wrists shows some
overlapping, so the sensitivity and specifity of US can not
accurately be assessed with this study.
Almost all previous studies of sonography in diagnosis of CTS
indicate an increase in cross section area of median nerve, with
a cut- off point of 10mm2 as the upper limit for normal values.
In our study, the dimension of tunnel itself was measured. We
found out the narrow anteroposterior carpal tunnel in severe
CTS, a finding which t has not been reported previously. It
seems people with a narrower anteroposterior diameter of carpal
tunnel are potentially more prone to develops CTS.
Conclusion:
Sonography is a useful
modality in diagnosis of severe CTS. We found out a decrease in
anteroposterior diameter of carpal tunnel in severe cases of
this disease. A finding which has not been considered
previously. This finding of narrow carpal tunnel may be
considered as a predisposing factor in severe CTS. To evaluate
the
US
results in mild to moderate disease, more study will be needed.
Reference :
1-
Phillip E. wright II. Carpal tunnel syndrome. In: Terry Canal S.
Campbell's Operative orthopaedics 10 the ed. Mosby. 2003;
3761-62.
2-
Brown feard tanzer: Entrapment neuropathies of the upper
extremity. In fly JE, el: Hand surgery...Ed 3
Baltimore
, 1982.william, s and wikins.
3-
Shirde AJ, Dreizint, and fisher MA: the carpal tunnel syndrome.
A clinical electrodiagnostic analysis, Electromyography. Clin
Neurophysio1981; l 21: 143.
4-
Gellman H,Gelberman RH tan AM, and Botte MJ:carpal tunnel
syndrome, an evaluation of the provocative diagnostic
test.J.Bone Joint sury.1986 ;63-A: 735
5-
Wong SM, Griffith JE, Hui AC. Discriminatory sonographic
criteria for the diagnosis of carpal tunnel syndrome. Arthritis
rheuma.jul 2002; 46-(7):1914-21.
6-
Duncan I, Sullivan P, loams F: sonography in the diagnosis of
carpal tunnel syndrome. AJR AMJ roentgenol. Sep 1999;
137(3):681-4.
7-
Sarria L, cabada T, Cozcolluela R, et al.Carpal tunnel syndrome:
usefulness of sonography.Eur Radiol.2000; 10(12):1920-5
8-
Buchberger W, Judmaier W, Birbamer G, et al: Carpal tunnel
syndrome: Diagnosis with high-Resolution sonography.AJR AM J
Roentgenol, Oct 1992; 159(4): 793-8
9-
EL.Miedany YM, Aty SA, Ashours: ultrasonography versus nerve
conduction study in patients with carpal tunnel syndrome:
rheumatology. (
Oxford
),Epub
Apr
2004; 887-95.
10-
Yesildag A, Kutiuhan N, Koyuncuogiu HP, el: the role of
ultrasonogruphy in the diagnosis of carpal tunnel syndrome.
Clini-racliol, Oct 2004; 59(10): 910-5
11-
Teefey SA, Middleton WD, Boyer Ml.sonography of the hand and
wrist. Semin Ultrasound CT MR, Jun 2002; 21(3):192-204.
12-
Kuo MH, Leong CP, Cheng YF, Chang HW. Static wrist position
associated with least median nerve compression: sonographic
evaluation evaluation. Am J Phys Med Rehabil. 2001 Apr;
80(4):256-60.
13-
Wilinand AA, Swen A, Johannres W G. Carpal tunnel sonography by
the rheumatolgist versus NCV by the neurologist, Journal
rheumatol 2001;28:62-9.
|

