| CASE
REPORT |
|
Tetraventricular
Hydrocephalus And Subarachnoid Fat Vesicles Induced By Ruptured
Spinal Dermoid Cyst
|
|
Mustapha
Maâroufi*, Imane Kamaoui*, Mohammed Benzagmout**, Saïd Boujraf***,
Siham Tizniti*
*Department
of Radiology,
University
Hospital
Hassan II,
Fez
,
Morocco
.
**Department of
Neurosurgery,
University
Hospital
Hassan II,
Fez
,
Morocco
.
***Department
of Biophysics and Clinical MRI Methods, Faculty of Medicine and
Pharmacy,
University of Fez
,
Morocco
.
Address for Correspondence:
Associate
Prof. Saïd Boujraf
Department of Biophysics and Clinical MRI Methods
Faculty of Medicine and Pharmacy,
University
of
Fez
BP. 1893; Km 2.200,
Sidi Hrazem Road,
Fez
30000
,
Morocco
Phone: 00 212 67 780 442, Fax: 00 212 35 619 321
E-mail: sboujraf@hotmail.com
|
|
Abstract:
The
authors report a case of spinal dermoid cyst which ruptured;
this originated a migration of free fat vesicles into the
ventricles and subarachnoidal spaces. The fat vesicles caused
obstructive hydrocephalus; witch represents a quite exceptional
complication. The intracranial fat causing hydrocephalus was
found before the discovery of the spinal mass. The authors
suggest that the finding of intracranial fat in the absence of a
local source makes the search for an intraspinal dermoid cyst.
J.Orthopaedics 2007;4(4)e23
Keywords:
dermoid, rupture,
free fat, hydrocephalus, MR imaging.
Introduction:
Free
fat in the brains cerebrospinal fluid (CSF) is recognized as
complication of ruptured intracranial dermoid tumors. On the
contrary, the diffusion of fat drops in intracranial CSF from
spinal dermoid cysts is unusual.
We
report a case of spinal dermoid cyst without associated spinal
dysraphism originating subarachnoidal, cisternal and
intraventricular fat drops. The fat deposits caused obstructive
hydrocephalus. In our case the finding of intracranial fat and
obstructive hydrocephalus preceded the discovery of the spinal
neoplasm.
Case report
A
35-year-old man, with a 1-year history of headaches, seizures
and a decrease of the general mental status. At the clinical
examination there was hyperreflexia of lower extremities. No
history of spinal trauma or lumbar puncture was registered.
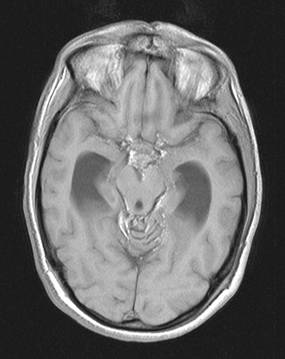
Cerebral magnetic resonance imaging (MRI) showed an obstructive
hydrocephalus with enlarged aqueduct due to fat drops that
probably obstructed the caudal portion of aqueduct, there was
another fat deposits located cisterna magna, cerebellopontine,
interpeduncular, and other basal cisterns (Figure 1). In the
absence of a local source of intracranial fat drops we performed
spinal MRI which revealed a large mass at the conus medullarus,
which was constituted of two portions: a cranial one, that was
tissular, isointense with the spinal cord on T1-weighted images;
and a caudal one that was fatty, showing higher signal on T1 and
T2 weighted images. Small subarachnoid fat deposits are present
at T7 and T9 level (Figure 2), linear high-signal area within
the distal spinal cord might represent syringomyelia, edema or
pericystic gliosis. On lumbar puncture, CSF protein and cells
were in a normal range. The patient underwent radical removal of
the spinal dermoid cyst of the conus medullarus, histologically
identified as a dermoid cyst.
Discussion :
Spinal
dermoid are rare benign congenital lesions (1-2% of all
intraspinal tumors) originating from inclusions of epithelial
elements within the neural groove at the time of its closure to
form the neural tube between the third and fifth weeks of
embryonic life [1].
About 25% are found in the sacrococcygeal region [2].
They may occur within the spinal cord.
The
clinical history is related to the lesion site, their slow rate
of growth allows reaching a considerable size even without
causing any symptoms.
Unless
insidious rupture occurs; the spillage of the keratin and
cholesterol products breakdown can generate variable symptoms
such as headache, dementia, seizures or transient cerebral
ischemia [3, 4]. Chemically
induced meningitis follows dermoid rupture with variable
clinical sequela. Symptoms of our patient can be explained by
the meningeal irritation by the spilled cholesterin materiel.
MRI
is the modality of choice for diagnosing the dermoid tumors; it
shows different components of a dermoid cyst, as well as small
free fat droplets in the subarachnoidal space. Dermoid cysts
usually present relatively homogeneous signal, higher than the
spinal cord on T1-weighted images. However, in some cases a more
heterogeneous pattern is observed, related to the composition of
the tumor. The relatively high signal from fat on MRI,
especially the bright signal on T1 weighting, makes for easy
identification of lipid droplets, particulary within the
cerebral sulci, fissures and the perimedullary subarachnoid
space. Fat droplets are rarely recognized on CT because of their
small size and their similar density to CSF on routine
windowing. The differential diagnosis of dermoid cysts on
imaging includes lesions with high lipid content such as
teratomas and lipomas.
Intracranial
fat spread originated from intraspinal dermoid rupture has been
recently emphasized [5, 6]. Our case is a further demonstration
of this possibility; witch indicates the interest of
complementary brain imaging examination of patients with
intraspinal dermoid, and vice-versa.
In
addition to generalized subarachnoid and ventricular spread of
droplets fat, our patient developed obstructive triventricular
hydrocephalus witch is an unusual manifestation [7]. The
hydrocephalus may be attributed to early alteration of
cerebrospinal fluid circulation by fatty materiel in the caudal
portion of cerebral aqueduct, and subsequent block by
subarachnoid fibrosis explaining the narrowing of this portion
[8, 9] (Figure 1).
|
|
|
|
Figure 1: Axial and
sagittal spin-echo T1-weighted image. Lipid droplets are present
in the cisterna magna, 3rd ventricle, interhemicerebral fissure
and schismatic cistern. A small droplet is seen in the caudal
portion of the cerebral aqueduct (arrow). The cranial portion of
witch is enlarged
|
|
|
|
 |
|
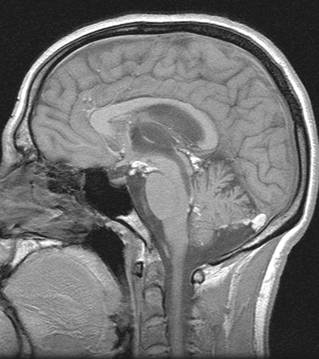
Figure 2: Sagittal
spin-echo T1 and T2-weighted images. An exophytic intramedullary
dermoid tumor is seen in the lumbar enlargement. The cyst has a
cranial portion that is solid and isointense with the spinal cord
(arrow) and a caudal portion giving high signal (arrowhead). Two
small lipid droplets are seen in the posterior subarachnoid space
at T7 and T9. Linear high-signal area within the distal spinal
cord may represent syringomyelia, edema or pericystic gliosis
|
|
Reference :
1.
Messori A, Polanara G, Serio A,Gambelli E, Salvolini U.
Expanding experience with spontaneous dermoid rupture in the MRI
era: diagnosis and follow-up. European Journal ol Radiology
2002;43:19-27
2.
Kavita K, Pankaj A, Sunil I. Dermoid of the conus medullaris.
Journal of clinical neuroscience 2004;11(7):796-797
3.
Karabulut N, Oguzkurt L. Tetraventricular hydrocephalusdue to
ruptured intracranial dermoid cyst. Europeen Radiology
2000;10:1810-1811
4.
Lunardi P, Missori P, Rizzo A, Gagliardi FM. Chemical meningitis
in ruptured intracranial dermoid. Case report and review of the
litterature. Surgical neurology 1989;32:449-452
5.
Barsi P, Kenez J, Varallyay G, Gergely L. Unusual origin of free
subarachnoid fat drops: a ruptured spinal dermoid
tumour.Neuroradiology 1992;34:343344.
6.
Calabro` F, Capellini C, Jinkins JR. Rupture of spinal dermoid
tumors with spread of fatty droplets in the cerebrospinal fluid
pathways. Neuroradiology 2000;42:572579.
7.
Cavazzani P, Ruella A, Michelozzi G, Andrioli G. Spinal dermoid
cyst originating intracranial fat drops causing obstructive
hydrocephalus: case reports. Surg Neurol 1995;43:466469.
8.
Scearce TA, Shaw CM, Bronstein AD, Swanson PD. Intraventricular
fat from a ruptured sacral dermoid cyst: clinical, radiographic,
and pathological correlation. Case report. J Neurosurg 1993;78:666668.
9.
Roeder MB, Bazan C, Jinkins JR. Ruptured spinal dermoid cyst
with chemical arachnoiditis and disseminated intracranial lipid
droplets. Neuroradiology 1995;37:146147.
|
|
This is a peer reviewed paper Please cite as
: Mustapha Maâroufi
: Tetraventricular
Hydrocephalus And Subarachnoid Fat Vesicles Induced By Ruptured
Spinal Dermoid Cyst
J.Orthopaedics 2007;4(4)e23
URL:
http://www.jortho.org/2007/4/4/e23 |
|
|

