|
Abstract:
Primary intramedullary anaplastic oligodendroglioma is a rare tumor.
We described a 27-year old male with primary intramedullary
anaplastic oligodendroglioma. He underwent partial removal of
tumor and spinal radiation therapy. The objectives were to
present a case of intramedullary anaplastic oligodendroglioma
and review the existing literature. A comparison of the
clinical, radiologic and pathologic characteristics, as they
relate to those already described in similar cases, was also
attempted.
Key Words: anaplastic oligodendroglioma, intramedullary
spinal cord tumor, radiation therapy
J.Orthopaedics 2007;4(4)e18
index.htm
Introduction:
Primary intramedullary oligodendroglioma is a
rare tumor and primary intramedullary anaplastic
oligodendroglioma is even more uncommon (1). Forty five cases of
primary intramedullary oligodendroglioma have been reported in
the literature till date and only five of these tumors were
anaplastic (1).
Case Report :
A twenty seven year old male presented to the
orthopaedics emergency with a history of lower back pain
radiating to the right lower limb associated with hypoesthesia
in the distribution of L5 and S1 dermatomes in the right lower
limb for the past 2 weeks. There was no preceding history of
trauma, constitutional symptoms such as low grade fever,
anorexia and weight loss. History of contact with a patient of
pulmonary tuberculosis was present. .His father had suffered
from pulmonary tuberculosis. On clinical examination, there was
tenderness at lumbosacral junction with paraspinal muscle spasm.
The straight leg raising test on the right side was 60 degrees
as compared to 90 degrees on the left side. Extensor hallucis
longus and extensor digitorum were weak (grade 4) on the right
side with sensory hypoesthesia in the L5 and S1 dermatomes.
Plain radiographs of the lumbosacral spine were normal. Based on
the history and clinical examination, a diagnosis of
intervertebral disc prolapse L4 - L5 was made and the patient
was advised bed rest and non-steroidal anti-inflammatory drugs.
He was even being considered for an epidural steroid injection.
Within a period of four days, the patient
deteriorated neurologically with involvement of left lower limb
and bladder as well. The muscle power in both the lower limbs
progressively deteriorated to grade three and eventually ended
in complete paraplegia with loss of control over bladder and
bowel. An ascending lumbar myelogram was performed and it
revealed complete block of the dye column at L1 level
(fig.1).Magnetic resonance imaging scan revealed an intradural
space occupying lesion opposite the bodies of D12 and L1
vertebrae. (Fig.-2).
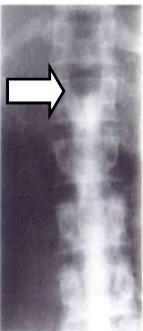
Figure 1:
Myelogram shows complete block of dye column at L1 level
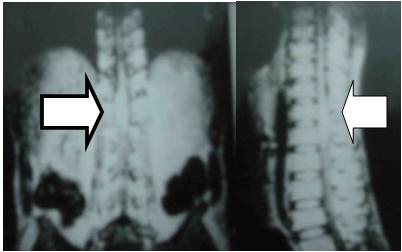
Figure 2:
MRI shows intradural space occupying lesion opposite the bodies
of D12 and L1 vertebrae
Laminectomy from D11 to L1 was performed. The
cord was found enlarged in a fusiform shaped swelling extending
from D12 to L1.On incising the dura; dirty black tissue
intermingled with the neural tissue bulged out. It was not
possible to remove the whole tumor tissue, a debulking surgery
was performed. The tissue was sent for histopathological
examination.
Histopathology sections showed a highly
cellular tumor with characteristic features of oligodendroglioma
with the tumor cells arranged in a lobular pattern. The cells
showed a perinuclear halo giving a honeycombed appearance to the
clusters of cells. Micro calcification was seen in areas. There
were foci suggestive of anaplasia with marked cytologic atypia
and considerable nuclear hyperchromasia. Another notable feature
was the presence of vascular hypertrophy and proliferation.
Areas of necrosis with pseudopalisading were seen in an
occasional field. (fig.3a, b). It was reported as an anaplastic
oligodendroglioma.
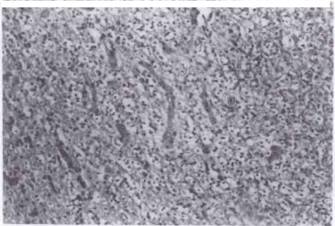
Figure 3 a: Shows an area of classical
oligodendroglioma with marked vascularity and endothelial
proliferation (200X)
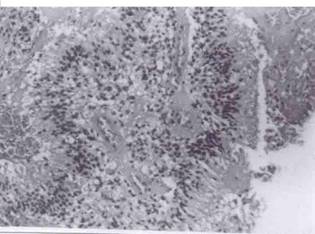
Figure 3 b:
Another field from the same tumor showing necrosis, vascular
proliferation and nuclear atypia (200X)
Postoperative
period was uneventful but the patient did not show any neural
recovery. He was referred to the radiotherapy department for
megavoltage radiotherapy. He did not report back to us. But
records of radiotherapy department say he is still following in
radiotherapy department at 16 months postoperatively.
Discussion:
Primary spinal
cord oligodendroglioma represents 0.8-4.7% of the tumors of the
spinal cord and filum and 1.59% of oligodendrogliomas (1). In
literature 5 cases of anaplastic oligodendroglioma of spinal
cord have been reported till date to the best of our knowledge
(1).
The peak age
incidence of oligodendrogliomas of the cord is around 30-40
years with no sex preference (2). In Fortuna et al series, three
of the reported cases were adults in the fifth decade and the
other was an 18 year old woman (3). Nam et al reported
anaplastic oligodendroglioma in a 38 month old boy (1). Our case
is a 27 year old male.
In the spinal
cord, approximately 30% of the tumors occur in the cervical
spine, 60% in the thoracic spine and 10% in the lumbar spine
(2). Out of the forty five reported cases of intramedullary
oligodendrogliomas only three were holocord i.e., extending over
nineteen to twenty cord segments (4). In our case, the tumor was
located at the dorsolumbar junction extending over two cord
segments i.e., D12-L1.
Most of the
patients present with pain, weakness and paraesthesiae
(3).Sphincter disturbances are never among the presenting
symptoms (3). Scoliosis may be the only sign of the tumor even
for several years without any other clinical sign. In addition
to these neural symptoms, primary intramedullary
oligodendroglioma has peculiar clinical characteristic of
preference for meningeal spread with intracranial hypertension
and fluctuation of symptoms owing to spontaneous bleeding (1).
The plain
radiographs may reveal indirect evidence of the lesion
(scalloping of the posterior vertebral bodies, erosion of the
pedicles, widening of the canal) (3). No such finding was seen
in our patient. Myelography usually reveals the diagnosis of an
intramedullary tumor (3). In our case, myelogram revealed
complete block of the dye column at L1 level. Magnetic resonance
imaging is the procedure of choice in the investigation of
spinal cord tumors. It can delineate tumor extension, though
edema may not be readily distinguished from neoplastic tissue;
gadolinium DTPA enhancement might help (4).
Surgical removal
and radiotherapy are the two described modalities of treatment
(3). Surgical removal may be complete or only debulking of tumor
if it is not possible to separate the tumor tissue completely
from the neural tissue. In each of the patients reported by
Fortuna et al and Nam et al, it was not possible to remove the
tumor mass in toto and a debulking procedure was done. In our
case too, a debulking surgery was done (3).
Macroscopically
oligodendrogliomas has been described in majority of cases as a
soft, gelatinous, infiltrating tumor, white or grayish pink in
color indicating greater clinical malignancy (3, 5). In a few
cases, the consistency of the tumor may be firm which is related
with a better prognosis (3). In the present case, the tumor
tissue resembled grayish, friable caseous material
preoperatively. Microscopically, the tumor presents a
honeycombed appearance (2). The cells are of uniform size and
shape and a clear halo around the nucleus is displayed in each
cell. Areas of calcification are frequently seen in
oligodendrogliomas. Increased mitotic activity and presence of
necroses are characteristically associated with an anaplastic
change (2, 5). All these features were noticeable in the
histopathology sections of the present case.
Radiotherapy is
an effective modality in primary malignant anaplastic
oligodendroglioma where considerable residual mass is left after
surgical debulking (1, 3, 6).We referred our case to
radiotherapy center for radiation therapy.
The prognosis of
primary intramedullary anaplastic oligodendroglioma in 4
reported cases was so poor that none survived for three years
(1). Radiation therapy may lead to a better prognosis (1, 3, 6).
In a child of 38 months the debulking was followed by
megavoltage radiation therapy and post radiation therapy MRI
revealed marked decrease in size and at 50 months after surgery
there was no evidence of progression (1). Thus once anaplastic
oligodendroglioma is diagnosed more radical therapy such as
craniospinal radiation with or without chemotherapy should be
given for a better prognosis.
Reference :
-
Nam
Do-Hyun, Cho Byung-Kyu, Kim Yeon- Mee et al: Intramedullary
anaplastic oligodendroglioma in a child. Childs Nervous
System, 14:127-130, 1998
-
Nathoo A.R.,
Halliday N.P.: Spinal cord oligodendroglioma. Postgrad Med J.,
43(506), 789-791, 1967.
-
Fortuna A,
Celli P, Palma L.: Oligodendrogliomas of the Spinal Cord. Acta
Neurochirurgica, 52:305-329, 1980.
-
Pagni C.A.,
Canavero S. Gaidolfi F.: Intramedullary Holocord
Oligodendroglioma: Case Report. Acta Neurochirurgica, 113:
96-99, 1991.
-
Russel D.S.,
Rubinstein L.J. : Pathology of tumors of the Nervous system.
Ed. 5,172-187, Baltimore, Williams and Wilkins, 1989.
-
Fountas KN, Karampelas I, Nikolakakos LG, Troup
EC, Robinson JS.: Primary spinal cord oligodendroglioma: case
report and review of Literature. Childs nervous system,
21(2):171-5, Feb 2005
|

