|
J.Orthopaedics 2007;4(4)e11
index.htm
Introduction:
Giant cell tumor is one of the most obscure and intensively
examined tumours of bone .its histogenesis is uncertain .the
histology does not predict the clinical outcome and there are
still many unanswered questions with regard to both its
treatment and prognosis
The World Health Organisation has classified GCT as "an
aggressive, potentially malignant lesion",which means that its
evolution based on its histological features is unpredictable.
Statistically, 80% of GCTs have a benign course, with a local
rate of recurrence of 20% to 50%. About 10% undergo malignant
transformation at recurrence and 1% to 4% gives pulmonary
metastases even in cases of benign histology
We present here an uncommon site for occurrence of the GCT in
the proximal femur, and its subsequent management. Approximately
50% of GCTs are located around the Knee at the distal femur and
proximal tibia1, 6, with the proximal humerus and
distal radius representing the third and fourth most common
sites. Mirra9 has reported an incidence of less than
4% of 1182 cases in this location.
Case Report :
A
male patient age 30 yrs presented to our hospital with h/o pain
in the right hip for six months duration. Radiating to the knee
joint. There were no significant lymphadenopathy and
neurovascular deficits. X rays of the LS spine taken and was
normal and pelvis with both hips showing osteolytic lesion in
the right trochanter.(fig1 )

FIG 1 . x
ray showing the osteolytic lesion at the proximal femur (trochanter)
CT scan was taken to see the extent of the lesion.
Histopathological report showed grade 2 (jaffe) giant cell
tumors 4 ( fig 2 & 3)
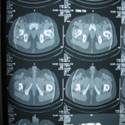
FIG 2. CT
scan showing extent of lesion
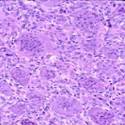
FIG 3.
histopathology showing the uniform distribution of osteoclast
like giant cells in a background of mononuclear cells
It
was operated with curettage and phenol cauterization and bone
grafting. He was followed regularly in our hospital for six
months with x rays to know the recurrence of lesion (fig 4)

FIG 4 . x ray after 1 st surgery curettage and bone
grafting
Later patient gave the h/o trivial trauma and inability to walk
after one year of surgery. X rays were taken which showed
recurrence of lesion with pathological fracture of the neck of
femur with lesion extending proximally to the middle of the neck
of femur and distally up to lesser trochanter .(fig 5)

FIG
5. x ray showing the recurrence with Pathological fracture
at the neck of femur without involvement of head
As the patient is young so we planned to preserve the head. So
we have done excision of the lesion with phenol cauterization
and fixed with 135O DHS and with bone cement. HPR also confirmed
the recurrence showing stromal cells with no appreciable atypism
and he was discharged and followed regularly (fig 6)

Fig
6. post op x ray with curettage, bone Cement and DHS post op
x ray with curettage, bone Cement and DHS
At present patient wounds were healed by primary intension and
there was no evidence of recurrence locally and patient does not
have any pain and walks normally and able to do routine
activities with full weight bearing
Range of movements flexion, abduction, rotations was
full. There was no limb, length discrepancy (fig 7)
Discussion:
In most benign aggressive bone tumours control can be achieved
by wide surgical excision .following en bloc resection, the rate
of the recurrence is in between 0% AND 5% in primary lesions
,because it is found in the epiphysis , the GCT often invades
the subchondral bone .en bloc resection often requires
sacrifice of the articular surface and s complex reconstruction
procedure ,which can lead to complications ,revision operations
and decreased quality of life in the long term .11 ,12
Resection is usually performed in GCT found in the proximal
fibula, radius, distal ulna, or in the wing of the ilium in
which a reconstruction is not necessary or in malignant types of
GCTs , stage -3 GCTs , which have already destroyed the cortex
tend to recur more often and when the defect is large an the
joint surface is destroyed , resection is indicated 10 11
.The treatment of choice in most GCTs is curettage and bone
grafting . Historically, however it has been associated with
high rate of recurrence (30%-50%) and therefore different
adjuvants have been introduced. these presumably remove the
tumour cell which remain after curettage because of their
thermal (liquid nitrogen, methylmethacrylate ) or chemical
(phenol , hydrogen peroxide ) effects ,3 6
11,12
.The
use of cement has advantages in that it is cheap, and immediate
weight-bearing is allowed. Furthermore, a local recurrence is
easily recognised around the cement both by radiographic and MR
investigations. Extended curettage and application of bone
cement are therefore the most accepted methods in the treatment
of GCT 10, 11
Treatment for this patient with recurrence had many options like
excisional arthroplasty like girdle stone7,
hemiarthroplasty8 or total hip arthroplasty8.
As results of hemiarthroplasty in young patients are poor and
well documented in literature5 8. And shortening and
prolonged immobilization is not accepted with excision
arthroplasty. As the patient was young we preferred to do a
joint sparing surgery with preserving the head with DHS. Phenol
cauterization was done as it is safe and effective local
adjuvant therapy with curettage as it is documented 3
and also the bone cement was used as it has been shown to
decrease the incidence of local recurrence in GCT 1,6.
The use of methacrylate leads to formation of a 2 mm osteolytic
zone surrounding it which is surrounded by sclerotic rim. Lysis
or failed development of the sclerotic zone adjacent to the
lytic zone is suspicious of recurrence which was not seen in our
case at the last follow up1 . Our case was grade II
jaffe4 histopathologically has no recurrence at the
last follow up
Reference :
1
Zhen,
W.; Yaotian, H.; Songjian, L.; Ge, L.; Qingliang, W.
Giant- cell tumour of bone: The long term
results of treatment by curettage and bone cement. Journal of
Bone & Joint Surgery - British Volume. 86-B (2):212-216, March
2004.
2. Lackman, Richard D MD; Hosalkar, Harish S MD; Ogilvie,
Christian M MD; Torbert, Jesse T MD; Fox, Edward J MD
Intralesional Curettage for Grades II and III Giant Cell Tumors
of Bone. Clinical Orthopaedics & Related Research. 438:123-127,
September 2005.
3. H R Durr, M Maier, V Jansson, A Baur and H J
Refior. Phenol as an adjuvant for local control in the treatment
of giant cell tumour of the bone .Eur J Sur Oncology , 1999 Dec
;25(6);610-8
4. Jaffe H L, Lichtenstein L, Portis RB. GCT of bone
, its pathological Appearance,Grading,Supposedvariants and
treatment .Arch Pathology 1940;30:993
5. Kulkarni SS, Dogra AS, Bhosle PB. Total hip
arthroplasty for giant cell tumour.J Postgrad Med 1996;42:82-4
6. Stefanp A, Bini,MD ;Kan Gill,MD ; and James O.
Johnston ,MD Giant Cell Tumors Of Bone curettage and cement
reconstruction .Clinical Orthopedics & Related Research number
321, 245-250,July 1995.
7. Harrison, M, H, M.Ch, FRCS Robert jones, Gathorne
Girdlestone and excision arthroplasty of the hip. Journal of
Bone & Joint Surgery-British volume, 87-B (9); 1306, September
2005.
8. Cannon, Christopher P MD;Lin,Patrick P MD;
Lewis,Valerae O MD; Yasko,Alan W MD . Acetabular Outcome after
Hip hemiartroplasty in patients with tumors. Clinical
Orthopaedics & Related Research, 20 November 2006.
9. Mirra JM Giant cell tumour .Mirra JM editor .bone
tumours, clinical radiological and pathological correlations
.vol.2. Philadelphia:lea and febier ;1989,pp942
10. McDonald DJ, Sim FH, McLeod RA, Dahlin DC. Giant cell
tumor of bone. J Bone Joint Surg [Am] 1986;68-A:235-42
11. O'Donell RKJ, Springfield DS, Motwani HK, et al.
Recurrence of giant-cell tumors of long bones after curettage
and packing with cement. J Bone Joint Surg [Am] 1994; 76-A:
1827-33.
12. Szendroi, M.Giant cell tumour of Bone. Journal 0f Bone
& Joint Surgery - British Volume. 86-B(1):5-12, January 2004
|







