|
J.Orthopaedics 2007;4(3)e16
Keywords:
Galeazzis variant fracture; ulnar nerve entrapment;
children
Background:
Fractures
of the distal radius in Children are common but a fracture of
the distal radius with a distal ulnar epiphyseal fracture and
anterior displacement otherwise known, as Galleazis Fracture
with ulnar nerve entrapment is very rare. In children such
fractures have been referred as a variant of Galleazzis
fracture. None of the previously reported Galleazis
equivalent fractures in children described the signs and
symptoms of ulnar nerve entrapment. In this case a small
fragment of the ulnar epiphysis was found to be the cause.
Case
Report :
A
17-year-old lad presented to A & E with dorsally angulated
fracture of left distal radius after having a fall from 7 feet
on to the outstretched left hand. On examination there was
dorsal deformity of the left wrist. There was no neurovascular
deficit at that time. X-rays confirmed the communited fracture
of distal shaft radius. A molded cast under sedation was applied
on the same day patient presented.
On
the first post-operative day, the patient complained of
paraesthesia in little finger and the ulnar border of ring
finger of left hand. Initially the impression was that the
symptoms of ulnar nerve compression were due to the very tight
plaster, it was released immediately, but the symptoms didnt
improve. On further review of X-rays a small fragment of ulnar
epiphysis was found to be displaced on volar aspect of the
wrist.
Figure
1. Missing fragment of distal ulnar epiphysis displaced
anteriorly over the volar aspect of ulna.
Open
reduction under anesthesia was carried out and the ulnar was
found entrapped in between the fragment of ulnar epiphysis and
distal ulna. The nerve was freed and ulnar epiphyseal fragment
was reduced and held in its original position with the help of 2
K-wires.
Three
weeks after the operation the patient was reviewed in fracture
clinic. Examination revealed complete loss of sensations in
ulnar nerve territory of left hand. No motor deficit was
detected. Re X-ray confirmed that the fixation has failed and
fragment has displaced. Hence, left wrist was re-explored via
extending the original incision under G.A. The ulnar nerve was
stretched tightly across the extruded fragment of distal ulnar
epiphysis and this fragment was mal-rotated. It was not possible
to reduce the fragment hence this was sacrificed allowing the
nerve to lie free. All wires were removed and wound was washed
out.
Figure
2.distal ulnar epiphysis displaces again after initial
reduction with the help of K-wires
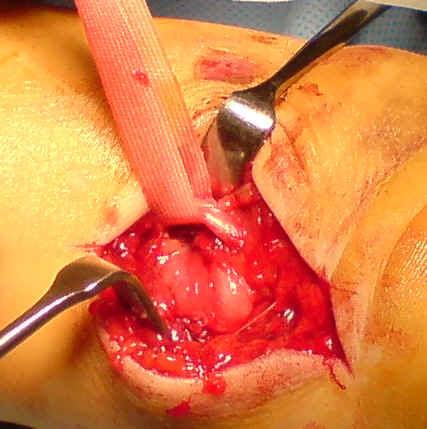
Figure
3.Ulnar nerve freed from the displaced ulnar fragment and
distal ulna
The
Pt. was followed up in the Out patient fracture clinic. He had
limitation of wrist extension by 5 degree, supination was
limited 10 degree but has full range of flexion and pronation.
The sensations in little finger gradually improved.
Discussion :
The classical
Galleazis fracture is defined as fracture of shaft of radius
with distal radioulnar joint dislocation but in children this
fracture has been referred as a Galeazzis Variant fracture
and it involves the ulnar epiphysis in place of distal
radioulnar joint. First description is by Reckling (1982). To
our knowledge there is no previous case reports in the
literature describing ulnar nerve entrapment in Galleazis
variant fracture. There are only few case reports mentioning
ulnar nerve involvement by multiple distal ulnar fragments but
none of these fractures are classed under Galeazzis variant
fracture²´³.
Our
case report is unique in a sense that its a Galeazzis
variant fracture involving ulnar nerve only by a single fragment
of epiphysis, which to our knowledge has not been reported
before. Another challenge in our case was that, the child was
only 17 years old and sacrificing the ulnar epiphysis may result
in arrest of growth plate but that was unadvisable. Five months
post injury the patient was regularly followed up and has now
been discharged from outpatient clinic with no signs of distal
ulnar growth arrest.
The
mechanism of injury in our case is somewhat similar to the
Galeazzis fracture i.e. fall on outstretched hand with
flexion at elbow but it is indeed very crucial to identify the
complications of Galeazzis equivalent fracture in children as
in our case there were two potential risks involved:
Arrest
of distal ulnar growth plate.
Loss
of ulnar nerve function.
Though
in our patient we initially missed the ulnar nerve entrapment
but as soon as we realized
Prompt
diagnosis is a key in the management of such fractures, if
delayed can lead to malunion with reduced function of the wrist
specially in children.
Reference :
-
Imatani J,
Hashizume H, Nishida K, Morito Y and Inoue H. The
Galleazi-equivalent lesion in children revisited. J hand
surgery [br] 1996 Aug; 21B (4) 455-7.
-
Saitoh S,
Koiwai H, Sensui K. Double type III epiphyseal separation of
distal ulna associated with ulnar nerve palsy. J ortho.
Trauma 1997 Feb-mar 11(2) 138-41.
-
Osada D, Tamai
K, Kuramochi T, Saotome K. Three epiphyseal fracture (distal
radius, Ulna and proximal radius) and diaphyseal ulnar
fracture in 7 year childs forearm. J of orthopedic trauma
2001 Jun-Jul; 15(5) 375-7.
-
Letts M,
Rowhani D. Galleazi equivalent injuries of the wrist in
children. J of orthopedics 1993; 13(5) 561-66.
|

