|
J.Orthopaedics 2007;4(3)e11
Introduction:
Septic arthritis may occur in patients of any age. The bacteria can
infect the joint by hematogenous route, by direct inoculation of
a wound or by direct extension of an adjacent osteomyelitis. The
most common causative agents of septic arthritis in elderly
people are Staphylococcus Aureus, β-Haemolytic
streptococcus and Gram negative bacteria such as Klebsiella and
Salmonella 1. The signs of septic
arthritis are fever, pain, swelling, heat, erythema and the loss
of joints movement.
Diagnosis is confirmed with biochemical examination and culture
of synovial fluid 1.
The main factor in determining the outcome of an infection is the immune
status of the host. The immune status can be weak by cancer,
diabetes mellitus, alcoholism, acquired immunodeficiency
syndrome, or corticosteroid therapy. Patients with nephrotic
syndrome are also immunocompromised hosts susceptible to
infections 2.
An extremely rare complication of nephrotic syndrome is the
development of septic arthritis. It is the first case of septic
Knee arthritis in literature which is caused by nephrotic
syndrome.
The most common bacterial agents developed in these patients are
Staphylococcus Aureus, Streptococcus Pneumonia and Escherichia
Coli 2.
However, other agents like Cryptococcus Neoformans 3
and Campylobacter Jejuni 4 are reported in patients
with nephrotic syndrome.
Several mechanisms of immunosuppresion have been reported 5,6.
The nephrotic syndrome is a disorder, and not a disease, where
the kidneys have been damaged. Its characteristic pentad is
massive proteinuria and that leads to hypoproteinemia
(hypoalbunemia), hyperlipidemia with elevated cholesterols,
triglycerides and other lipids, and edema.
We present a
case of septic knee arthritis, caused by staphylococcus Aureus in
a 68-year-old man, as an
extremely rare complication of nephrotic syndrome.
Case
Report:
A
68-year-old man has visited our hospital, complaining of acute
knee pain without previous trauma, for the last 24 hours. On
physical examination we found erythema, swelling and high
temperature over his left knee. The
general symptoms were
temperature 38,7oC, malaise and anorexia.
There was an unknown history of nephrotic
syndrome, although the patient mentioned mild periorbital and
ankle edema in the last month. He mentioned the continued
receipt of anti-inflammatory drugs for the last two months,
because he suffered from a tendonitis of supraspinatus muscle,
as well. His laboratory
results were: White Blood Cells 18000/mm3 with 82%
polymorphonuclear cells, C - reactive protein 27,9mg/dl and
Erythrocyte Sedimentation Rate 76mm/h. Uric acid, Rheumatoid
factor, antinuclear antibodies, C3 and C4 were negative. A knee radiograph and computer tomography scan showed
degenerative changes of osteoarthritis. (Figure 1 a, b, c).

Figure
1. a. Clinical view of infection of the Knees joint

Figure 1. b.
X-ray
anteroposterior view shows degenerative changes of
osteoarthritis.
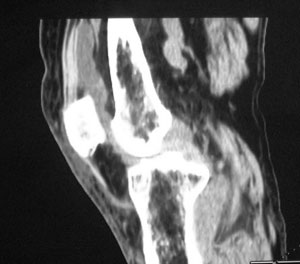
Figure 1.c.
CT of the Knee did not show any bone abscess.
Joint aspiration was performed and synovial fluid was taken for
biochemical examination and cultures. Synovial fluid was turbid
and purulent. Methicillin Resistant Staphylococcus Aureus was
isolated from the culture of synovial fluid. For the isolation
was used sheep blood agar 5%. Synovial fluid analysis with the
biochemical parameters analyzer Cobas
Integra 800 (Roche,Basel,Switzerland) showed White Blood Cells
78000/mm3, with 80% polymorphonuclear cells, protein
3,6gr/dl and glucose 26mg/dl.
We did not detect the existence of nephrotic syndrome and septic
knee arthritis was initially treated with arthroscopic
debridment. We started intravenous antibiotic therapy,
consisting of 1gr Vancomycin twice daily, according to
antibiogramma, as well.
The
symptoms were the same after one week therapy. The patient
was screened meticulously and we found serum albumin 2,4g/dl,
albumin in urine 4,6gr/24h, cholesterol 288mg/dl and
triglycerides 230mg/dl, which revealed
the diagnosis of nephrotic syndrome.
The
nephrotic syndrome was treated by nephrologists and we continued
the intravenous antibiotic therapy for 3 weeks. The joint was
immobilized in a cast for 1 week and after that we started
continuous passive movement. After one week of therapy the
condition of the patient improved slowly. The local signs, the
sedimentation rate and C reactive protein levels had
returned to normal. The antibiotic therapy was continued by an
intramuscular injection of teicoplanin daily for other 3 weeks.
The patient was followed-up for 18 months and he did not show
any clinical sign of recurrence.
Discussion :
The morbidity and mortality of acute septic arthritis are significant
especially at young children and elderly people. Bone
and cartilage destruction are the main complications of septic
arthritis in adults. The knee joint is the most frequent
affected. Septic arthritis of the hip, shoulder, ankle, wrist,
elbow, tarsal, sacroiliac, acromioclavicular and
sternoclavicular joints is less frequent 1.
Diagnosis is documented with analysis of blood and synovial
fluid parameters. The isolation and identification of pathogen
microorganism confirm the infection. Age is an important
factor in determining the causative microorganism of septic
arthritis. The most common microorganisms found in elderly
people are Staphylococcus Aureus, β-Haemolytic streptococcus
and Gram negative bacteria such as Klebsiella and Salmonella 7.
Staphylococcus Aureus is the causative agent in the half of
these patients 7.
The
joint can be infected by direct invasion, by blood spread from
another site or by direct spread from a adjacent bone abscess 1.
The most causative organisms of septic arthritis in people with
immune deficiencies are Mycoplasma, Staphylococcus,
Streptococcus, and Haemophillus 8.
Soft tissue infections, due to immune system disorder, can occur in
nephrotic syndrome. Nephrotic patients have increased risk of
infection because of several mechanisms. The fluid collections
help bacteria to grow easily, dilute local humoral immune
factors and in combination with the fragile skin create sites of
entry. Also the loss of IgG, complement and factor B reduce the
ability to eliminate encapsulated organisms 2.
This is the first case of septic Knee arthritis in literature which
caused by nephrotic syndrome. We
treated the patient, according to the three principles of the
treatment, with antibiotic therapy in combination with
arthroscopical debridment and rest of the joint in a stable
position 1. The isolated microorganism was MRSA and
we used according to antibiogramma Vancomycin. This antibiotic
is the primary choice for the treatment of MRSA 9.
Arthroscopic drainage and debridment is an alternative treatment
for the knee and other joints like shoulder, elbow and ankle 1.
The debridment must be performed within 72 hours from the
initial symptoms. Fibrinoid
material and infected debris can be removed with lavage. After
the acute stage of infection, the passive movement of the knee
should be start. The early continuous passive movement prevents
the adhesions and helps the nutrition of the cartilage, during
the healing phase of septic arthritis 10. The patient
must use crutches for 2 weeks.
However, in our case this treatment did not have good results, initially.
So, the
patient was
screened meticulously for other abnormalities because there was
not a history of a previous trauma. We found
hypogammaglobulinemia, increased loss of albumin with urine, and
high rates of cholesterol and triglycerides, which revealed
the diagnosis of nephrotic syndrome.
The main sign in nephrotic patients is edema. The
patient had reported mild periorbital and ankle edema in the
last month, but this element was not evaluated properly. Either
previous joint trauma or
past medical history of arthritis increases the risk of septic
arthritis development.
When nephrologists treated the nephrotic syndrome, the patients
condition was improved. We though that in our patient,
hypogammaglobulinemia caused by nephrotic syndrome, was the main
cause of immune system defect with total IgG less than 180mg/dl and one of the main factors of maintenance of infection. This reason is
responsible for the fail
of initial therapeutic strategy.
In septic arthritis of unknown origin, nephrotic syndrome should be
considered among one of the causes. This case is the first
description in literature of septic Knee arthritis which was
developed in a patient with nephrotic syndrome.
Reference :
- Park LA, Dlabach
AJ. Infectious
arthritis In: S.Terry Canale eds. Cambpells operative
orthopaedics, 10th ed.
St Louis
: CV Mosby-Year book Inc., 2003: 685-689.
- Johnson RJ,
Rennke H, Feehally J. Introduction
to glomerular disease: Pathogenesis and classification. In: Johnson RJ and
Feehally J eds. Comprehensive clinical Nephrology, 2th ed.
St Louis
: CV Mosby Co, 2003: 255-269.
- Qadir F.
Disseminated Cryptococcosis in a patient with
nephrotic syndrome. Indian J Med Microbiol. 2006; 24(2):
141-143.
- Simon CH,
Markusse HM. Campylobacter Jejuni Arthritis in secondary
amyloidosis. Clin Rheumatology. 1995 Mar; 14(2):214-6.
- Fiser R.T,
Arnold W.C, Charlton R.K, Steele R.W, Childress S.H, Shirkey
B. T-lymphocytes subsets in nephrotic syndrome. Kidney Int.
1991;40 :913-6.
- Matsumoto K,
Osakebe K, Hatano M. Impaired cell-mediated immunity in
idiopathic membranous nephropathy mediated by suppressor
cells. Clin Nephrology. 1983; 19(4) :213-4.
- Stimmler MM.
Infections arthritis: tailoring initial treatment to
clinical findings. Infect Arthritis. 1996; 99: 127.
- Sordet C, Cantagrel A, Schaeverbeke T, Sibilia
J. Bone
and joint disease associated with primary immune
deficiencies. Joint Bone Spine. 2005 Dec;72(6):503-14.
- Hamed KA, Tam
JY, Prober CG. Pharmacokinetic optimization of the treatment
of septic arthritis. Clin
Pharmokinet. 1996; 31(2):156-63.
- Salter RB,
Bell
RS, Keeley FW. The protective effect of continuous passive
motion on living articular cartilage in acute septic
arthritis: an experimental investigation in the rabbit.
Clin Orth Relat Res.
1981; (159):223-47.
|

