|
Abstract:
To research a new method to treat the
fracture and nonunion of the region from anatomical neck to the
diaphysis part of the proximal humerus. According to the
mechanical character of bio memory material Nitional and the
physiological character of proximal humerus, a new device called
proximal humerus memory connector was designed. 22 cases of comminuted fracture,
malunion and nonunion of proximal humerus were treated by this
device. The healing style was characterized by plate bone
substitution, no disordering callus was observed. The function
of the shoulder was scored average 88.5 according to the
criteria of Michael Reese. PHMC is an efficacious method to treat
every type fractures and nonunion of the region from anatomical
neck to the diaphysis part of humerus, and a new way is explored to reduce the rate of
prostheses displacement of this part.
Keywords: Humeral fractures; Shoulder fractures; Proximal humerus
memory connector
J.Orthopaedics 2007;4(2)e38
Introduction:
The
4-5% of all the fracture is the fracture of proximal humerus
[1-2].For dislocated comminuted fracture of proximal humerus ,
the steel plate and bolt system made of the austenitic material
sometimes is difficult to find point of resistance force in
order to maintain restitution and fixation effectively,and
furthermore the ununited fracture and ischemic necrosis of caput
humeralis are common[1,3]. Conservative treatment often leads to
pain and different degrees of disability because of metachoresis
and compareed long-term external fixation[4,5] So the reports of
the prosthetic replacement are seen frequently[6]. Owing to
this, the author invents the proximal humerus memory
connector(PHMC),according to the characteristic of the nitinol
alloy [7]and the anatomic figure of proximal humerus .from
August 2000 to September 2003, total 22 cases of fracture
malunion and ununited fracture of proximal humerus had been
treated by PHMC. Now we reports as follow.
Design,principle and application
The Structure Design
According to the anatomic and biomechanical features of proximal
humerus, choosing 2 to 2.5mm thickness nickel 50at%~53at%
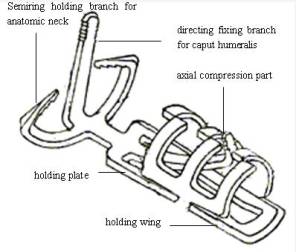
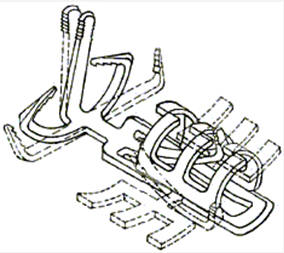
nitinol plate, the PHMC is designed to consist of head part,
axial compression part and body part(see fig.1). The head part
consists of directing fixing branch for caput
humeralis and humerus semiring holding branch for anatomical
neck. The holding plate and holding wing compose body part.It is
treated to have one way memory effect and recovery temperature
is 33±2℃. According to the fracture type, The PHMC is designs
to typeⅠand type Ⅱ.Each type consists of different
sizes.
The Principle
The head body and compression part are deformated in low temperature to
fit the figure of operation region on proximal humerus.The
metallography of PHMC is changed by body temperature,which leads
to mechanics proceeding. (1) Directing fixing branch and semiring
holding branch stabilize disclosed caput humeralis. (2) The
standard body part will hold the non-standard tubular bone
on with multipoint fixation. The hooks of axial compression
parts will be inserted into the holes on two side of the
fracture. (3)The directing fixing branch and compression branch which are
restricted by the bone hole when reverting to their original
shapes exert continuously memory compressure at the fracture
line. Because of above mentioned 3 reasons, PHMC and two ends will compose 3D mnemonic
fixation.
The Method of Application
According to the type,of fracture, the type
and size of PHMC are decided before operation. General
anaesthesia or block anaesthesia of brachiplex is applyed.
Semirecumbent position is taken . Anteriomedial approach of
shoulder is chosed . The incision can be extended to acromial
process if necessary. The incision to ilium is prepared.
(1)The fracture of greater
tubercle lesser tubercle and surgical
neck or anatomical
neck of humerus. The fracture site is explored ,a bone
channel which diameter is 0.4-0.6 cm is drilled on the site
0.5-1.0 cm below the tip of greater tuberosity of humerus,
casting shadow to the center of caput humeralis and not
piercing through articular facet. And then the directing
fixing branch of the PHMC is inserted into the channel. The
points for semiring holding branch inserting are determined, the
pores are drilled ,and then the branches are inserted into the
pores. The head part of PHMC is rewarmed. And then, the body
part of PHMC is inserted, the holding wings fix the distal end of
fracture, and PHMC is rewarmed. At last, the points for axial
compression part which is plastic formed and expanded are
determined , the pores are drilled ,and then the part is
inserted into the pores. The part is rewarmed. So the whole
fixation is completed.
(2)
The
nonunion of surgery neck of humerus. The scar and free
bone sequestrum are removed to expose the cancellated bone of
the proximal end of the nonunion. The medullary cavity of distal
end is drilled through. Then the PHMC is applyed. At last, the
holding wing of PHMC is cooled and spread out of bone. The iliac
grafting bone composed of cancellated bone and cortical bone is put into the space between bone and
PHMC, which spanned the fracture site like splints. The
cancellated bone is towards the nonunion while the cortical bone
is towards the PHMC. Finally, PHMC is rewarmed and fixes the
nonunion.The spatium between PHMC and bone is filled with scum
of spongy bone.
(3)
The serious comminuted fracture or
compressed defection of greater
tubercle lesser tubercle and surgical
neck of humerus.
The large surface of iliac bone graft is taken to contact the
cancellated bone of cancellated bone ,while the small end of the
graft is inserted into the medullary cavity of distal diaphysis.
(4) The serious
comminuted fracture or compressed defection of greater
tubercle lesser
tubercle and surgical neck and comminuted
fracture of proximal 1/3 diaphysis
of humerus.
At
first comminuted fracture of diaphysis is reduced and fixed by
arched toothed nails from far distally to proximum; The
subsequent processes are applyed according to above (3) (1).
(5) The articular capsule
and rotator cuff
can be tied to the semiring holding branch for anatomical neck
of humerus.
Postoperative Management
(1) Drainage. A drainage will be retained for
24~48h in cases of fractures and nonunion.
(2) stopping. Suspension with triangular bandage for one
week generally.
(3) Functional exercise.
About 2 days after operation, the patient should begin to
contract the muscle group of upper arm actively and
gradually.And about 2 weeks after operation, the patient should
begin to flex or extend the shoulder actively and gradually.
(4) Removement
of PHMC.
10-18 months after operation, PHMC can be removed by
choosing the primary incision, refrigerating PHMC, then prying
the hooks of compressing branch and semiring holding branch, and
spreading the wings at last.
Results :
Clinical
result:
Common Information
Total 22 cases include comminuted fracture malunion and ununited fracture
of proximal humerus were treated by PHMC.There are 13 cases of
fracture ,involving greater tubercle lesser tubercle surgical
neck and anatomic neck,4 cases of malunion and 5 cases of
ununited fracture among them. There were 15 males and 7 females.
The age ranged from 13 to 69 years (arerage 41.7 years);
Result
All cases were followed up from 6 to 37 monthes,
average 18.5 months. The fracture attained synostosis at an
average time of 3.6 monthses ,and the ununited fracture was at
4.5 monthses. All the fracture sites were replaced by lamellar
bone,and there were no disordered bony callus .External fixation
was not needed after operation by PHMC.After trauma response
(about 7-12 days after operation), the patient should begin to
functional exercise actively and gradually. The average score of
shoulder joint function is 88.5 according to the criteria of
Michael Reese [9]
Conclusion:
3D Biomechanic Characteristics of
PHMC[10-13]
(1) The directing
branch of head part
and the semiring holding branch outside the articular capsule
and the axial compression part
provide the mnemonic compressive stress that does not
disappear because of absorption of fracture line. It can provide
dynamic stimulus for the ossification.
(2) The stabilization of multiple points providing
by difference between internal diameter of PHMC and external
diameter of bone belongs to the 3D stabilization of non- axis
and non- side wall.
(3)
The patient can do functional exercise actively and gradually
after trauma response (7-12 d). so the PHMC not
only
can stabilize bone
pieces, but also can accustom
the straining of
the muscle group on the place .
The Indication of
PHMC
The
various fracture
and nonunion of the region from anatomical neck to the diaphysis
part of the proximal humerus.
The Characteristic and
Management of Above Region
On one hand, comminuted fracture of
the region usually have different compressed cancellous defect. On the other hand, cortical bone of the
surgery neck is thin. So it is difficult to find fixing location
if crashed. There is more hollow yellow marrow on surgical neck
of the old, so it is difficult to get supporting locoation to
reunion if crashed. These characteristics put forward the
problems how to apply bone graft. The tips for bone graft are as
follows.
(1) Building up the fulcrum of defection. The iliac
bone block is chiseled from the site 4cm behinds anterior
superior iliac spine, extending 2-3cm along iliac crest
backwards, then descending 4cm down. So the bone graft is about
4cm long and 2-3cm wide. The crest of iliac bone graft is
broadest position of iliac bone graft . The cancellated bone of
it is exposed.The large surface of iliac bone graft is taken to
contact the cancellated bone of cancellated bone. Another end of
iliac bone graft is trimmed the same size of the medullary
cavity and inserted into the cavity.
(2) Filling up the space surrounding the defection
The space between PHMC and bone is filled with mixed scum of
ilium and recombinated heterogeneic bone.
(3) Build up the exterior anatomic form of the
defection. The bone stick spanned the defection like splints,
clamped by bone holding wing.
Above 3 points fits the case of nonunion,too.
Comprehensive treatment is applied to the special case showed by
fig.5 and fig.6.
The Characteristic of Fixation and Ossification of PHMC
The 3D mnemonic dynamic mechanic environment of PHMC,
the characteristic of bone graft and the anatomic figure of
proximal humerus effect each other.which creats multipolar 3D
force field. The difference of diameter between PHMC and bone
and multipoint fixation promote the recovery blood supply. The
mnemonic compression between fracture site promotes the
ossification. All the fracture sites were replaced by lamellar
bone,and there were no disordered bony callus. This kind of
healing appears accompanying with the active and gradual
functional exercise after trauma reaction.The unification of
valid fixation, ossification, function recovery is attained on
the whole [10,11].
The Clinical Significance of PHMC
For
the fracture of the region from anatomical neck to the surgical
neck of the proximal humerus,the prosthetic replacement is
recommended more and more frequently. The reason is as follows.
At first,It is difficult to fix this kinds of fracture by plate
and/or tension band; On the orther hand, Kuner etc.[14]
report the rate of ischemic necrosis of caput humeralis
is 44.6% for the fracture of proximal humerus fixed by plate,
the rate is 33.3% for the fracture limited fixed by
screw tension band and polydimethylsiloxane(PDS).
The result of prosthetic replacement caused by ischemic necrosis
for the old is fair, but for the young, the problem caused by
replacement also allows of no
optimism[15]. The result of study shows the PHMC can make
the fracture attain anatomic reduction and bone healing, There
is no report of ischemic necrosis so far. Certainly, we still
needs the long-term observation on the big sample, but at least
the case showed by fig.4 is worth us more exploration and
thought.
The Limitation of PHMC
The PHMC is not suitable for compressed comminuted
fracture of the region from anatomical neck to the caput
humeralis. How to fix this kind of fracture effectively, reduce
the prosthetic replacement and recover the function as soon as
possible is still a topic that needs to continue to approach.
References :
-
Browner, D. et al, Skeletal trauma(English copy)1st
, Science Publisher (Bei Jing, 2001). pp. 1570-1571.
-
Qu, W., Wang, S. F., et al,. Treatment of fracture of proximal humerus by AO LPHP.,J China Trauma, vol 19
(2003), pp,625-627.
-
Kocialkowski, A., Wallace, W. A., Closed percutaneous K-wire
stabilization for displaced fractures of the surgical neck of
the humerus. Injury, vol 21,(1990), pp,209-212.
-
Stableforth, P. G., Four-part fractures of the neck of the humerus.
J Bone Joint Surg (Br), vol 66,1984, pp,104-108.
-
Moda S K, Chadha N S, Sangwan S S, et al. Open reduction and fixation
of proximal humeral fractures and fracture-dislocations. J
Bone Joint Surg (Br), vol 72 (1990), pp, 1050-1052.
-
Lin, H. S. ,Zha ,Z .G., Wang ,G .J ,et al, Treatment for coplex
fracture of proximal humerus by artificial caput humeralis. J
China Trauma, vol19,( 2003), pp,410-412.
-
Otsuka, K, Wayman ,C.M. ,Shape memory materials. (Translated by Zhang ,C.
C, Su ,J C, et al).1st. Smmu
Publisher (Shang Hai 2003). pp, 189-197.
-
Arched toothed memory bone connector(type I),PRC. Patent ZL 01 3 44222.8
-
Dai ,K.R.,e t al, Surgeryof shoulder 1st.
Peoples Health Publisher, (Bei Jing1992) pp, 401-403.
-
Zhang ,C. C., Xu ,S.G., Wang, J. L .,et al. Design and clinical
applications of swan-like memory-compressive connector for upper
limb diaphysis, Tans of smmu,vol22(2001),pp,939-942.
-
Zhang,C.C.,Xu,S.G., et al. Design and clinical applications of
swan-like memory-compressive connector for upper limb diaphysis.
Material Science Forum 2002, pp, 33-36.
-
Xu,S.G.,Zhang,C.C.,Su,J.C.,et al. The vitodynamic study of the
treatment of ununited fracture and fracture of humerus by swan-like memory-compressive
connector. Tans of smmu,vol22(2001),pp,946-948.
-
Xu,S.G.,Zhang,C.C.,Su,J.C.,et al. The 3D finite element analysis of
the treatment of ununited fracture and fracture of humerus by swan-like
memory-compressive connector. Tans of smmu,vol22(2001),pp,943-945
-
Kuner ,EH, Siebler G. Luxationsfrakturen des
proximalen Humerus---Ergebnisse nach operativer
Behandlung---Eine AO-Studie über 167 Fälle.Unfallchirurg,
vol.100, ( 1987), pp,64-71.
-
Speck M, Regazzoni P. Vier-Fragment-Frakturen des
proximalen Humerus: Alternative Strategien der chirurgischen
Behandlung. Unfallchirurg, vol. 100, ( 1997), pp, 349-353.
|