|
Dattatray
Kale*, Arun A Salunkhe#, Hemant P Parekh**, Mukesh*, Shripad
Joshi*,Prashanth A*
*
Resident
#Ex Hon Associate Professor
** Lecturer
Dept Of Orthopaedics, B.J. Medical College,Pune
Address for Correspondence:
Dr Hemant P Parekh
Lecturer ,Dept Of Orthopaedics
B.J. Medical College, Pune
Phone: 9225500848
E-Mail: dr_hemantparekh@yahoo.com
|
|
Abstract:
Background-
The success of management of DDH depends on early diagnosis so
that it can be treated with conservative methods with excellent
outcome. Late diagnosis may require surgical interventions which
are associated with complications e.g. avascular necrosis. X ray
diagnosis of DDH depends on appearance of ossific nucleus of
capital femoral epiphysis at about six months of age.The aim of
our study was to analyse the role of USG in early screening of
DDH in infant and whether selective screening of infants with
high risk factors for DDH is more yielding and cost effective as
compare to screening of all the infants.
Methods
- A prospective study was undertaken to screen 100 infants
(50 with risk factors and 50 without the risk factors for the
DDH) with USG between 2004 and 2006. We have used Grafs alpha
and beta angle measurements for the diagnosis,typing and
treatment of DDH.All the infants were followed up to the age of
24 months of age.
Results-
We detected six abnormal hips from the first group (infants
with risk factors) and two abnormal hips from the second group
(infants without risk factors). Four hips from the first group
required the treatment according to Grafs guidelines. Rest of
the two hips from the first group and both the hips from the
second group matured without treatment. Excellent results are
seen in all the patients at 24 months of follow up.
Conclusion-
In conclusion,we have found that USG screening by Grafs
method is very useful for early diagnosis of DDH. In countries
like India, where incidence of DDH is low ,selective screening
of infants with risk factors for the DDH has higher case
detection rate and hence more cost effective.
Keywords:
DDH- Developmental dysplasia of hip; USG- Ultrasonography;
Grafs method; High risk screening
J.Orthopaedics 2007;4(2)e33
Introduction:
DDH
is primrarily an acetabular dysplasia leading to subluxation or
dislocation at birth or few weeks to months following birth. Its
incidence in western population is 1/1000 live births. In India
its incidence is low but exact figures are not available due to
lack of large screening studies by USG.
In
pre USG era the definitive diagnosis of DDH was possible with x
ray at about 6 months of age. But the acetabular cartilage
growth potential is maximum in first four months. Thus (with x
ray) diagnosis is delayed and conservative methods of treatment
may not work. USG can detect catilagenous acetabulum and capital
femoral epiphysis 4, therefore very useful in early
diagnosis of DDH 1. With early diagnosis majority of
cases can be treted conservatively. Early treatment makes full
use of maturation potential 4 of acetabular cartilage
and excellent results can be expected.
Prof
Graf 4 on the basis of his fouty years of experience
has deviced USG method for early diagnosis, typing 5
and treatment of DDH. In our study we compared USG screening of
infants with risk factors for the DDH with those without the
risk factors.
Aim
of our study was to assess the role of USG in early screening of
DDH and to decide whether selective screening of infants with
risk factors for DDH is more cost effective or not.
Material and Methods :
A
prospective study of USG screening of hip joints of 100 infants
is conducted between 2004 & 2006. Two groups were formed
Group
I: 50
infants with risk factors for DDH
Group
II: 50 infants
without risk factors for the DDH.
We
included following risk factors for the DDH
1
female sex
2
breech presentation
3
associated anomaly eg.
CMT,CTEV,CDK
4
abnormal clinical findings- unequal gluteal folds, limited hip
abduction, positive Galeazzi sign, positive
Ortolini/Barlow tests.
 |
 |
| Table 1 |
Table 2 |
 |
 |
| Figure 1 |
Figure 2 |
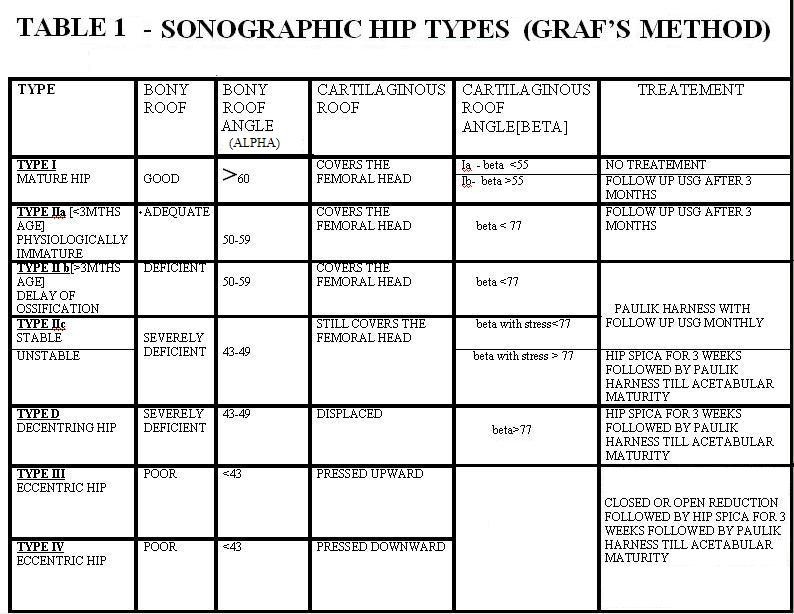
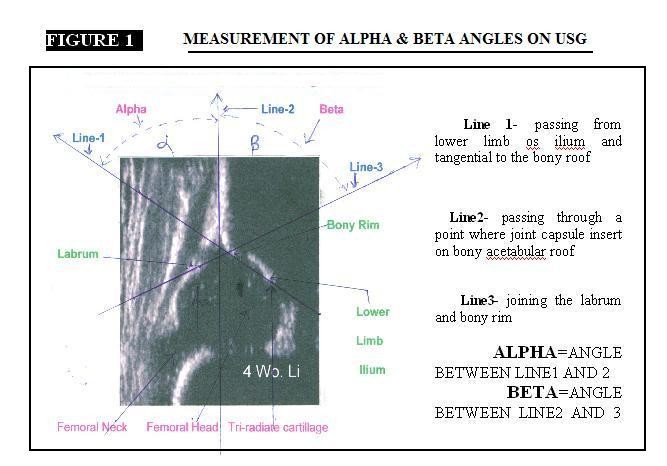
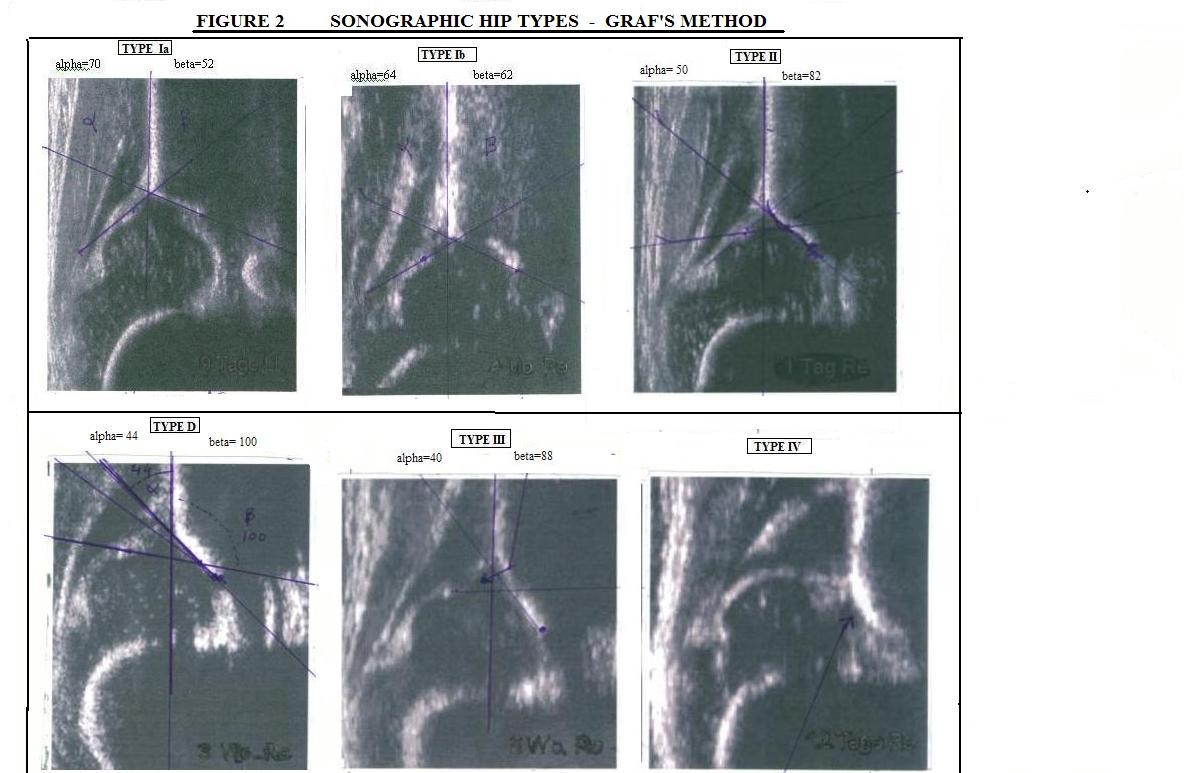
We
have used Grafs alpha and beta angle4 measurements
for the diagnosis,typing 5 and treatment of DDH.
First screening is performed between 0-3 months of age. Further
follow up was done clinically,radiologically and sonographically
till the age of 24 months.
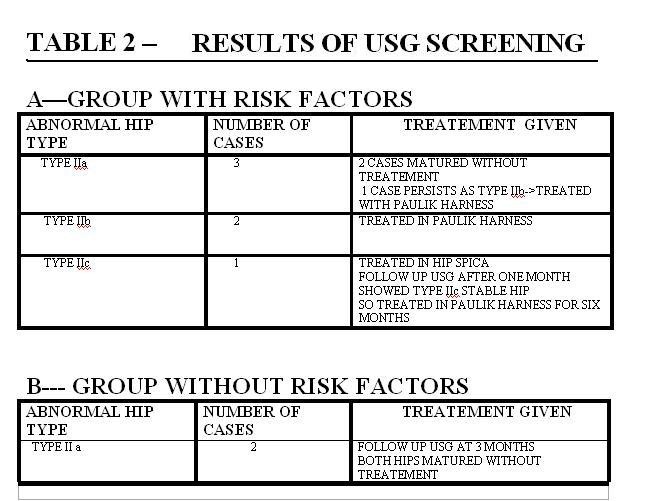
Results :
We detected six abnormal hips from the first group
(infants with risk factors) and two abnormal hips from the
second group (infants without risk factors). Four hips from the
first group required the treatment according to Grafs
guideline. Rest of the two hips from the first group and both
the hips from the second group matured without treatment.
Excellent results are seen in all the patients at 24 months of
follow up
Discussion :
This
study projects the utility of USG in early detection of DDH. The
success of outcome of DDH depends on early institution of
management by early detection. Lately diagnosed cases often
require surgical correction with its attendent complications. A
missed case of DDH can be disaster for the patient. As the
disease affects girls more frequently, in the countries like
India such girls face problems during marriage.
Review
of literature shows many studies supporting role of sonography
in early screening of neonatal hip for DDH 2,4,6,9,10. There are
studies favouring high risk screening 3,8,11 and studies against
it 7. .A study by Zenios M ( U. K.) 12 recommends screening of
all the neonates with USG where as study by Giannakopoulou C
(Greece) 3 recommends selective USG screening of high risk
neonates only.
In
our study we tried to compare the results of screening of infant
hips with risk factors for DDH with those without the risk
factors. In the screening of 200 infant hips , 8 hips were found
to be abnormal [ 6 hips (6%) from the high risk group and 2 hips
(2%) from the control group]. Four hips required treatment while
four hips(less severe affection) matured without treatment. All
have excellent results on clinical,radiological and sonographic
follow up conducted till the age of 24 months.
Limitations
of our study - i)Larger follow up is needed. ii) most of
the type IIa hips under three months of age matures to type
I(normal hip) at three months of age. That means USG
overdiagnose and hence overtreat type IIa hips (80% in our
series). However if first screening is done at or after 3 months
of age it delays the diagnosis and hence treatment of type IIc
hips.Therefore the early screening is justified. iii)we have not
followed up the cases with normal USG ,therefore can not predict
false negativity of the screening test. iv) our sample size is
small, therefore can not predict the incidence rate of DDH.
To
conclude we have found that USG screening by Grafs method is
very useful for early diagnosis of DDH. In countries like India,
where incidence of DDH is low, selective screening of infants
with risk factors for the DDH has higher case detection rate (6%
as against 2% ) and hence more cost effective.
Reference :
-
De Pellegrin M, Tessari L.Early ultrasound diagnosis of
development dysplasia of the hip.: Bull Hosp Jt. Dis. 1996;54
(4): 222-5. 65
-
Davids JR, Benson LJ, Mubarak SJ, McNeil N.Ultrasonography and
development dysplasia of the hip: a cost-benefit analysis of
three delivery systems. J Pediatr Orthop. 1995 may June: 15(3)
325-9. 70:
-
Giannakopoulou C, Aligizakis A, Korakak E,Neonatal screening for developmental
dysplasia of the hip on the maternity wards
in
Crete, Greece. correlation to risk factors. Cllin Exo obstet
Gynecol. 2002;29 (2) 148-52, 23
-
Graf R :The
diagnosis of congenital hip dislocation by ultrasonographyArch
Orthop Trauma Surg 1980; 97: 117-33 (Medicine)
-
Graf R
:Classification of hip joint dysplasia by sonography Arch Orthop
Trauma Surg 1984; 102: 248-55
-
Graf R , Tschauner, Klapsch W. Progress in prevention of late DDH by
sonographic newborn screening-results of comparative follow up
study. J Pediatr Orthop B 1993;
2:115-21
-
Paton RW,
Srinivasan MS, Shah B, Hollis S.Ultrasound Screening for hips at
risk in developmental dyaplasia. Is it worth its?J Bone Joint
Surg. Br. 1999 Mar;81 (2):255-8. 44:
-
Sosendahl K, markestad T, Lie RT Cost- effectiveness of alternative screening
strategies for developmental dysplasia of the hip. Arch Pediatr
Adloesc Med. 1995 Jun; 149 (6) 643-7. 69:
-
Terjesen T, Bredland T, Berg V.Ultrasound for hip assessment in the
newborn.J Bone Joint Surg Br. 1989 Nov; 71(5) : 767-73. 108:
-
Wirth T, Startmann L, Hinrichs F.Surgical procedures after 14 years of
neonatal ultrasound screening. J Bone Joint Surg. Br. 2004
May ; 86(4):585-9. 13
-
Walter RS,
Donaldson JS, Davis CI,Ultrasound screening of high-risk
infants. A method to increase early detection of congenital
dysplasia of the hip. AM J Dis Child . 1992 Feb; 146 (2):230-4.
102:
-
Zenios M, Wilson
B, galasko CS,The effect of selective ultrasound screening on
late presenting DDH.J pediatr Orthop B. 2000 Ocr;9(4):244-735
|