|
The capsule of the
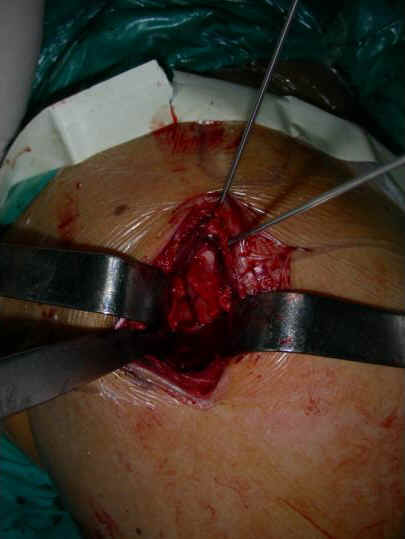
shoulder was longitudinally opened. The hematoma among the
fragments was cleaned and fracture fragments were identified.Firstly the impacted humeral head was elevated using two 2.5mm
K-wires inserted into the humeral head and then reduce the
greater tuberosity to humeral head. The reduction of the humeral
head to humeral shaft was performed with manual traction.TLastly
the arm was external rotated and the displaced lesser tuberosity
was reduced. In each step, the reduction was provisionally
maintained with k-wires and then determined with image
intensifier on the AP scapular view (fig2). Once the fractures
have been reduced, a sub-deltoid muscular
tunnel was made by small elevator and a locking proximal
humeral plate (LPHP) was introduced beneath the deltoid. The
proximal end of the plate was located posterior to the greater
tuberosity ridge and inferior to the articular surface of the
humeral head. A 2.0mm K-wire was used to fix the proximal end of
plate to humerus through wire hole. The adequate positioning of
the distal end of plate to the humeral shaft was adjusted and
confirmed by an additional small incision made on the lateral
arm using a same LPHP as template (fig 3a). The distal end of
the plate was temporally fixed to the humeral shaft with a
K-wire through a screw hole and more K-wires were used to fix
the proximal end of plate through wire holes. The reduction and
the position of plate were re-evaluated by image intensifier on
the AP scapular view and axillary view (fig 3b). Four locking
screws were used to fix the proximal end of plate to the
proximal humerus and three conventional cortical screws were
applied to the distal end of plate through the small incision or
percutaneously. The last position of fragment, plates and the
length of screws were confirmed with image intensifier after all
the K-wires were removed. The possible torn rotator cuff tissues
were repaired and the wound was closed as usual.
|

|
|
| Fig.1 An incision was started
from a point 1.5cm anterior to the lateral rim of the
acromion |
Fig.2 The fractures were reduced
and provisionally fixed with K-wire |
Postoperative
management included in 4- to 6-week protection of affected arm
with neck-wrist sling. The active range-of-motion exercises of
the shoulder and elbow were encouraged immediately after
operation, especially the abduction and external rotation of the
shoulder.
2.3.
Follow-up
All
the patients were followed up by clinical and radiographic
assessment. The operation time was defined as time from skin
incision to skin closure. Also recorded were the hospital stay
after operation, the time of bone healing, sensation of the
lateral arm, complications and functional outcome of shoulder,
especially the active motions in anterior flexion, abduction,
external rotation and internal rotation were recorded.
Radiographic
assessment was made by conventional anteroposterior scapular,
lateral scapular, and axillary views.
The
union was defined with the presence of a bridge callus in two
views, and AVN was defined with loss of bony substance and
presence of diffuse sclerotic area in the humeral head. Malunion
was defined if there was a displacement of more than 5 mm or an
angulation of more than 40 degrees of any fragment. The results
were evaluated using the Constant Shoulder Scoring system [14].
|

|

|
|
Fig. 3a An other LPHP was used as a template to
identify the most distal screw hole |
Fig.3b a stab incision was made and a 2.0mm K-wire was inserted into
the distal hole(b). |
Results :
 The mean operation time was 143.75±38.81min (range 80-240min).
The mean hospital stay after surgery was 7.31±2.41days
(range2-12 days). No local complications were observed. One
patient was lost. Fifteen patients were followed-up with mean
time of 6.1 months (range 5-14 months). All the fractures were
united with mean duration of 14.85 weeks (range 8-19 weeks). The
sensitivity of lateral shoulder is normal. There was no failure
of internal fixation. No AVN has occurred yet. The latest
visited result showed 120-170 degrees of active anterior flexion
(average 150.42 degrees) of the shoulders (fig 4). According to
Constant-Murley scoring system, the mean score of the shoulder
was 76.82 points (range 59-89.5 points), 4 patients had
excellent results, 5 good results, 6 moderate.
The mean operation time was 143.75±38.81min (range 80-240min).
The mean hospital stay after surgery was 7.31±2.41days
(range2-12 days). No local complications were observed. One
patient was lost. Fifteen patients were followed-up with mean
time of 6.1 months (range 5-14 months). All the fractures were
united with mean duration of 14.85 weeks (range 8-19 weeks). The
sensitivity of lateral shoulder is normal. There was no failure
of internal fixation. No AVN has occurred yet. The latest
visited result showed 120-170 degrees of active anterior flexion
(average 150.42 degrees) of the shoulders (fig 4). According to
Constant-Murley scoring system, the mean score of the shoulder
was 76.82 points (range 59-89.5 points), 4 patients had
excellent results, 5 good results, 6 moderate.
Discussion :
The
anterolateral aspect of the shoulder is covered with the middle
and anterior head of the deltoid muscles originated from the
inferior surface of the lateral third of the clavicle, acromion
and innervated by anterior branch of the axillary nerve. The
axillary nerve arises from posterior
cord of brachial
plexus and passes through the quadrangular space in
company with the posterior humeral circumflex artery and then
divides into anterior and posterior branches. The anterior
branch winds around the surgical neck of the humerus, beneath
the deltoid, with averaged 22 degrees of angle superior to the
perpendicular of the humerus axis. The anatomic studies have
demonstrated that the anterior branch of the axillary nerve
transverse the interval between the anterior and middle portions
of deltoid muscle and the average distance from the undersurface
of the acromion to the superior border of the nerve measured
63.3mm(range53.2-70.4) and the nerve can also elevated from the
lateral cortical surface at least 10mm without placing tension
on the nerve [11].
Therefore,
when the anterolateral approach was applied to reduce and
stabilize proximal humerus fractures, the length of the incision
should be kept within 60 mm. Besides, when sub-deltoid muscle
tunnel was prepared for pass through LPHP, the height of the
tunnel should not exceed 10mm so that the axillary nerve could
be protected from injury.
In
our case series, when the patients were lastly visited, the
sensory examination of the lateral arm was normal. The contour
of the shoulder as well as the strength of the anterior and
middle potion of the deltoid muscle were not significant
affected, indicated that it is security to accomplish the
reduction and fixation of the proximal humeral fractures through
the small anterolateral shoulder incision.
Gardner
et al [11] recommended the extended anterolateral incision in
which the axillary nerve was first dissected and protected. We
don not think that it is necessary to dissect the nerve only to
avoid iatrogenic axillary nerve injury. It will increase the
risk of nerve injury and take long operating time. In fact, in
the first two patients, the nerve was carefully dissected and
protected, but in remaining patients only the neurovascular
bundle was partially exposed. According to Bono et al [15] , the
distance from the lateral prominence of the greater tuberosity
to the superior edge of axillary nerve was 35.5mm (range
32.1-42.5), and the distance from the surgical neck to the
axillary nerve was 17 mm (range7-40 mm). This limits is large
enough to reduce the fragments, drill the hole and insert four
locking screw at the proximal plate.
In
obese patient whose fractures were difficult to expose through
the small incisions, the nerve should be dissected. In that
condition, only the neurovascular bundle was exposed. There was
no necessary to free the nerve completely. But for very fatty
patient, the deltopectral approach was recommended.
We
prefer to use the small elevator to prepare the sub-muscular
tunnel and keep the tip of the elevator close to the cortical
surface of lateral humerus so that the risk of the nerve injury
was decreased. The periosteum beneath the nerve was stripped and
the tip of the elevator was not exceeded about 5mm distal the
nerve. The remaining part of the tunnel was prepared using LPHP.
According
to Horak et al [16], the majority of the proximal humerus
fractures were the two part, the three and four part fractures
represent 13% to 16% of all the fractures. Most of them could be
reduced by indirect or close methods [4, 17, 18] except to the
greater tuberosity, which could be reduced on the direct
visualization through the incision. The Neer type IV fractures
are associated with the impacted humeral head and widened joint
space. Resch et al [3] recommended a method to reduce the head
with an elevator advanced into the gap between the greater and
lesser tuberosity and beneath the head and raised the impacted
head. We reduced the impacted the humeral head using two 2.0mm
K-wires drilled in the head after slightly distracting the
displaced greater and lesser tuberosities toward lateral and
medial side respectively. The impacted humeral head was then
slowly elevated through the two K-wires while one assistant
maintained the traction along the longitudinal axis of upper
extremity. The elevated head was temporally fixed to the humeral
shaft using one K-wire inserted from lateral side of humeral
shaft or from the head. The displaced greater tuberosity was
then reduced. The reduction of the lesser tuberosity was carried
out by external rotation of the arm.
Under the assistant of image intensifier combined with
direct and indirect reduction technique, the proximal humerus
fractures even if the four part fractures could also be
anatomically reduced through this small incision.
In
comparison with the deltopectoral approach, open reduction and
internal fixation of the proximal humeral fractures through the
anterolateral access has advantages of small incision; more
direct to expose the fractures, less damages to soft tissue and
less time needed to expose the fracture. More importantly, it
may reduce the damages to the blood supply to the fragments and
thereby decrease the risk of avascular necrosis of humeral head.
According to Hesmann et al [19], when the fracture was reduced
indirectly the incidence of avascualr necrosis of humeral head
is significant low. In our case series, all the procedures
including the exposure and reduction of the fragments,
introduction of the plate and screws adhere to the principles of
minimal invasive techniques and therefore promoting the
rehabilitation and the union of the bone.
In this case series, the mean operating time is 143.75min,the
mean time of bone union is 14.85weeks and the mean time of
hospitalization after surgery is 7.31days. The overall clinical
results, with a mean Constant and Murley score of 76.82 points
in patients with an average age of 45 years are comparable with
the results reported by Frankhause et al[10,20]. None of our
patients had a non-union and failure of implants.
LPHP
is locking plate exclusively designed for treatment of proximal
humerus fractures [21]. It is not necessary to mold the plate
intraoperatively because the size and contour of the plate are
matching with appearance of lateral aspect of the proximal
humerus. The size of LPHP is small with thickness of only 2.0mm.
The distal end of plate is taper-shaped so that it can be very
easily inserted sub-muscularly and passed by fracture site at
the epiphysis. It is a guarantee of MIPO technique and easier to
apply .The reduction of the fragments of the proximal humerus
could be firmly maintained with the angular stability between
the locking screws and the proximal end of the plate. There are
also 6 wire holes in the proximal end of the plats used to fix
the small fragments of proximal humerus to the plate with
sutures or wires when necessary. In this series, the four
locking screws and three conventional screws were applied to the
most proximal and distal screw holes on the plates leaving the
others intact to avoid the nerve injury. If it necessary to
insert the screws at these holes the percutaneous techniques
were selected.
Conclusion:
In this case series
of proximal humerus fractures, the advantages of LPHP were
adequately fulfilled. The fractures were exposed and reduced
directly through the small incision. The distal end of the plate
was positioned sub-muscularly and fixed to the humeral shaft
with percutaneous screws orientated with a same LPHP as
template. Obviously, it is LPHP that made the possibility to
treat the proximal humerus fractures with open reduction and
internal fixation through the anterolateral small incision in
the shoulder. It should be a good method to apply LPHP through
the small anterolateral incision of the shoulder to treat the
proximal humerus fractures
Reference :
1.
Kristiansen B, Kofoed H. Transcutaneous reduction and
external fixation of displaced fractures of the proximal humerus.
J bone Joint Surg (Br) 1988: 70B: 821-4.
2.
Ko JY, Yamamoto R. Surgical
treatment of complex fracture of the proximal humerus. Clin
Orthop Relat Res. 1996;(327): 225-37.
3.
Resch H, Povacz P, Frohlich R, Wambacher M. Percutaneous
fixation of three- and four-part fractures of the proximal
humerus. J Bone Joint Surg Br. 1997;79(2): 295-300.
4.
Qidwai SA. Treatment of
proximal humeral fractures by intramedullary Kirschner wires. J
Trauma. 2001; 50(6): 1090-5.
5.
Adedapo AO, Ikpeme JO. The results of
internal fixation of three- and four-part proximal humeral
fractures with the Polarus nail. Injury. 2001; 32(2): 115-21.
6.
Wachtl SW, Marti CB, Hoogewoud HM, Jakob RP, Gautier E Treatment of
proximal humerus fracture using multiple intramedullary flexible
nails. Arch Orthop Trauma Surg. 2000; 120(3-4): 171-5.
7.
Hessmann M, Baumgaertel F, Gehling H, Klingelhoeffer I, Gotzen L. Plate fixation of
proximal humeral fractures with indirect reduction: surgical
technique and results utilizing three shoulder scores. Injury.
1999; 30(7): 453-62.
8.
Esser RD. Open reduction and internal fixation of three-
and four-part fractures of the proximal humerus. Clinical
Orthoppaedics and Related Research 1994;299: 244-245.
9.
Robinson C M, Page RS, Hill RMF, Sanders DL, Court-Brown
CM, Wakefield AE. Primary hemiarthroplasty for treatment of
proximal humeral fractures. J bone Joint Surg Am. 2003; 85-A:
1215-1223.
10.
Fankhauser F, Boldin C, Schippinger G, Haunschmid C, Szyszkowitz R. A new locking plate for unstable fractures
of the proximal Humerus. Clin Orthop Relat Res, 2005;430:
176-181.
11.
Gardner MJ, Griffith MH, Dines JS, Briggs SM, Weiland AJ,
Lorich DG. The extended anterolateral acromial approach allows
minimally invasive access to the proximal humerus. Clin Orthop
Relat Res.2005; 434: 123-129.
12.
Gallo RA, Zeiders GJ, Altman GT. Two-incision technique
for treatment os complex proximal humerus fractures. J Orthop
Trauma 2005;19: 734-740.
13.
Neer CS II. Displaced proximal humeral fractures. Part I.
Classification and evaluation. J Bone Joint Surgery Am.
1970;52:1077-1089.
14.
Constant CR, Murley AH. A clinical method of functional
assessment of the shoulder. Clin Orthop 1987;214:160-164.
15.
Bono CM, Grossman MG, Hochwald N, Tornetta P 3rd.Radial and
axillary nerves. Anatomic considerations for humeral fixation.
Clin Orthop Relat Res. 2000;373: 259-64.
16.
Horak J, Nilsson BE. Epidemiology of fracture of the
upper end of the humerus. Clin Orthop 1975;112:250-3.
17.
Chen CY, Chao EK, Tu YK, Ueng SW, Shih CH. Closed management
and percutaneous fixation of unstable proximal humerus
fractures. J Trauma. 1998;45(6):1039-45.
18.
Williams GR Jr, Wong KL.Two-part and
three-part fractures: open reduction and internal fixation
versus closed reduction and percutaneous pinning. Orthop Clin
North Am. 2000;31(1):1-21.
19.
Hessmann
M, Gotzen L, Gehling H, Baumgaertel F, Klingelhoeffer I.Operative
treatment of displaced proximal humeral fractures: two-year
results in 99 cases. Acta Chir Belg. 1998;98(5):212-9.
20.
Bjorkenheim JM, Pajarinen J, Savolainen V. Internal
fixation of proximal humeral fractures with a locking
compression plate: a retrospective evaluation of 72 patients
followed for a minimum of 1 year. Acta Orthop Scand.
2004;75(6):741-5.
21. Frigg R. development of the locking
compression plate. Injury (Suppl 2) 2003; 34:6-10.
|

