|
Abstract:
Localised
Langerhans-cell histiocytosis of bone (eosinophilic granuloma)
is a benign tumour-like condition with a variable clinical
course. Different forms of treatment have been reported to give
satisfactory results. Although the mechanism of action of
intralesional injection of a corticosteroid has not been
defined, use of percutaneous needle biopsy to diagnose localized
Langerhans-cell histiocytosis and treatment with intralesional
administration of methylprednisolone relieved pain
expeditiously, enabled the patient to avoid an operative
procedure, and resulted in osseous healing. Right Ilium was
involved in a 3 year old boy. CT guided biopsy revealed
eosinophilic granuloma. Intralesional
steroid instillation was done, lesion healed well with no
recurrence after 7 years follow up.
Keywords: Eosinophilic
Granuloma, Pelvis, Intralesional steroid
J.Orthopaedics 2007;4(2)e25
Introduction:
The
clinical spectrum of Langerhans-cell histiocytosis (LCH) is
wide, ranging from a potentially lethal leukaemia-like disorder
to a solitary lytic lesion of bone10. Localised LCH of bone is a
benign tumour-like condition which is characterised by a clonal
proliferation of Langerhans-type histiocytes20, and is commonly
referred to as eosinophilic granuloma12. The bones which are the
most commonly involved are the skull, the pelvis, and the
diaphysis of long bones18. The systemic condition includes Hand-Schüller-Christian
disease with a triad of exophthalmos, diabetes insipidus and
osteolytic lesions of the skull, and Letterer-Siwe disease with
hepatosplenomegaly, lymphadenopathy, skin rash, fever, anaemia
and thrombocytopenia12.
Case
Report:
3year
old boy presented to us with pain & swelling in right iliac
region of 2 months duration. History of irregular fever and
unable to bear weight on affected limb. The child was on
antibiotic treatment before coming to our centre - being treated
as osteomyelitis.
ON
EXAMINATION:
-
Right Hip in 30° fixed flexion deformity.
-
Severe tenderness over Right Iliac crest and
gluteal region.
-
Severe painful restriction of (Rt) hip movements.
-
No distal Neurovascular Deficit.
-
General and systemic examination was normal.
[FIGURE 1]
X-RAY:
Pelvis revealed large Lytic lesion in Right Iliac bone [FIGURE
2] Serum Alkaline Phosphatase: 200 IU/L, rest all laboratory
investigations were within normal limits.
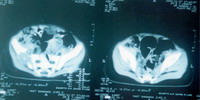
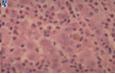
CT
scan reveled osteolytic lesion of the right ilium [FIGURE 3 AND
4]. At the same sitting CT guided FNAC was done with a wide bore
needle. FNAC revealed Sheets of langerhan's cells. These cells
are derived from the mononuclear cell and dendritic line
precursors Cytoplasmic inclusion bodies --birbeck's granules
suggestive of eosinophilic granuloma [FIGURE 5].
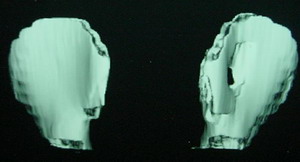
Patient
underwent a single dose of intralesional 120 mg of methyl
prednisolone acetate instillation. Pain free and improved
movement at hip with ability
to bear weight with
in 3 weeks .Patient was followed periodically and there was
total obliteration of the lesion at the end of 7 year follow up
[FIGURES 6 AND 7] with no recurrence.
 |
 |
| Fig 1 |
Fig 2 |
 |
 |
| Fig 3 |
Fig 4 |
 |
 |
| Fig 5 |
Fig 6 |
 |
| Fig 7 |
Discussion :
Localized
Langerhans-cell histiocytosis of bone (eosinophilic granuloma of
bone) is a rare, benign tumorlike condition that is
characterized by a clonal proliferation of Langerhans-type
histiocytes 11,12,13,19. Although the etiology and
pathogenesis remain unknown, the clinical course is usually
benign but can be highly variable, with partial or complete
healing of the lesion, recurrence after treatment, or
progression or spontaneous remission without treatment 3,4,5.
Radiographically,
the differential diagnosis includes osteomyelitis and Ewing
sarcoma in children and metastatic carcinoma and other benign
and malignant primary tumors of bone in adults. The diagnosis
must be confirmed with operative (open) or percutaneous biopsy.
Osseous
healing has been observed after various therapeutic
interventions, including curettage or low-dose radiation
therapy, or both5,14,16,17; intralesional injection
of corticosteroids2,7,8,9; and oral chemotherapy 21.
Intralesional
injection of corticosteroids is a non-operative approach that
has been demonstrated to produce rapid relief of pain with
predictable healing and without the need for additional
intervention 2,7,8,9.
Although
the precise mechanism of action of intralesional injection of
methylprednisolone for the treatment of localized Langerhans-cell
histiocytosis has not been defined, to our knowledge, several in
vitro studies have demonstrated the production of interleukins
(such as IL-1 [interleukin-1]) and prostaglandins (such as
prostaglandins E2 and D2) by suspensions
of Langerhans cells 1,6. The inhibition of
IL-1-induced bone resorption and prostaglandin production by
methylprednisolone may account for the dramatic response
demonstrated both clinically and radiographically15.
Conclusion:
It is extremely
difficult to establish guidelines for the treatment of a rare
condition such as Langerhans-cell histiocytosis. The least
invasive procedure appropriate for the level of expertise at a
given institution. Intralesional steroid instillation when used
gives rapid resolution of symptoms and in radiographic evidence
of healing of the osseous lesions without recurrence.
Reference :
-
1.
Arenzana-Seisdedos, F.; Barbey, S.; Virelizier, J. L.;
Kornprobst, M.; and Nezelof, C.: Histiocytosis X purified (T6
sup +) cells from bone granuloma produce interleukin 1 and
prostaglandin E sub 2 in culture. J. Clin. Invest., 77: 326-329,
1986.
-
2. Capanna R, Springfield DS, Ruggieri P,
et al. Direct cortisone injection in eosinophilic
granuloma of bone: a preliminary report on 11 patients. J
Pediat Orthop 1985;5:339-42.
-
3.
Chacha, P. B., and Khong, B. T.: Eosinophilic granuloma of bone.
A diagnostic problem. Clin. Orthop., 80: 79-88, 1971.
-
4.
den Herder, B. A.: Changing views on eosinophilic granuloma of
bone. Radiol. Clin. Biol., 42: 218-221, 1973.
-
5.
Fowles, J. V., and Bobechko, W. P.: Solitary eosinophilic
granuloma in bone. J. Bone and Joint Surg., 52-B(2): 238-243,
1970
-
6.
Gonzalez-Crussi, F.; Hsueh, W.; and Wiederhold, M. D.:
Prostaglandins in histiocytosis-X. PG synthesis by histiocytosis-X
cells. Am. J. Clin. Pathol., 75: 243-253, 1981.
-
7.
Jones, L. R.; Toth, B. B.; and Cangir, A.: Treatment for
solitary eosinophilic granuloma of the mandible by steroid
injection: report of a case. J. Oral and Maxillofac. Surg., 47:
306-309, 1989.
-
8.
Katz, R. L.; Silva, E. G.; DeSantos, L A.; and Lukeman, J. M.:
Diagnosis of eosinophilic granuloma of bone by cytology,
histology, and electron microscopy of transcutaneous
bone-aspiration biopsy. J. Bone and Joint Surg., 62-A:
1284-1290, Dec. 1980.
-
9.
Kindy-Degnan, N. A.; Laflamme, P.; Duprat, G.; and Allaire, G.
S.: Intralesional steroid in the treatment of an orbital
eosinophilic granuloma [letter]. Arch. Ophthalmol., 109:
617-618, 1991.
-
10. Ladish S, Jaffe ES. The
histiocytocis. In: Pizzo PA, Poplack DG, eds. Principles
and practices of pediatric oncology. Philadelphia: J. B.
Lippincott Company, 1989:491-504
-
11.
Lichtenstein, L.: Histiocytosis X: integration of eosinophilic
granuloma of bone, "Letterer-Siwe" and "Schuller-Christian
disease" as related manifestations of a single nosologic
entity. Arch. Pathol., 56: 84-102, 1953.
-
12. Lichtenstein L. Histiocytosis X
(eosinophilic granuloma of bone, 'Letterer-Siwe disease and
Schuller-Christian disease'): further observations of
pathological and clinical importance. J
Bone Joint Surg [Am] 1964;46-A:76-90
-
13.
Lichtenstein, L., and Jaffe, H. L.: Eosinophilic granuloma of
bone. With report of a case. Am. J. Pathol., 16: 595-604, 1940.
-
14.
Makley, J. T., and Carter, J. R.: Eosinophilic granuloma of
bone. Clin. Orthop., 204: 37-44, 1986.
-
15.
Marusc, A., and Raisz, L. G.: Cortisol modulates the actions of
interleukin-1 alpha on bone formation, resorption, and
prostaglandin production in cultured mouse parietal bones.
Endocrinology, 129: 2699-2706, 1991.
-
16.
McCullough, C. J.: Eosinophilic granuloma of bone. Acta Orthop.
Scandinavica, 51: 389-398, 1980.
-
17.
McGavran, M. H., and Spady, H. A.: Eosinophilic granuloma of
bone. A study of twenty-eight cases. J. Bone and Joint Surg.,
42-A: 979-992, Sept. 1960.
-
18. Nesbit ME Jr. Bone tumours in
infants and children. Paediatrician
1972/73;1:273-87.
-
19.
Schajowicz, F., and Slullitel, J.: Eosinophilic granuloma of
bone and its relationship to Hand-Schuller-Christian and
Letterer-Siwe syndromes. J. Bone and Joint Surg., 55-B(3):
545-565, 1973.
-
20. Willman CL, Busque L, Griffith BB, et
al. Langerhans histiocytosis (histiocytosis X): a clonal
proliferative disease. New Eng J Med
1994;331:154-60
-
21.
Womer, R. B.; Anunciato, K. R.; and Chehrenama, M.: Oral
methotrexate and alternate-day prednisone for low-risk
Langerhans cell histiocytosis. Med. and Pediat. Oncol., 25:
70-73, 1995.
|

