|
Keywords: Patella, Ilizarov, Quadriceps lag
J.Orthopaedics 2007;4(1)e12
Introduction:
Patellar fractures
account for 1% of all skeletal fractures.1 Due to the
central role of the patella in ensuring
continuity of the extensor mechanism, therefore salvage of the
patella is indicated in all but
the most severely comminuted fractures. The goal of all surgical procedures in the
management of patellar fractures is to accurately reconstruct
the extensor mechanism.Non Union of the
fracture of the patella is rare with a reported incidence of
2.4%.2 Non union is well tolerated
by patients with limited or decreased functional demands on the
knee. This however is
not true in cases with a large gap between the fragments.
Reports about the management of
such situations are even rarer.3
We report the case of
an eight month old non union of a patellar fracture in a 60 year
old male with a significant
gap between the fragments. Preliminary application of the
Ilizarov technique to bring the
fragments together helped avoid possible complications during final surgery.
Case
report:
A 60 year old male
reported to the outdoor department of our hospital with
inability to walk unaided. On
eliciting the history, the patient revealed that he had
sustained a trauma to the knee 8 months
ago due to fall from a height. He had been unable to walk
unaided since then and had
started using a cane to move around one week after the trauma.
The patients pain had
subsided over a period of 3 weeks, by which time he had become habituated and reliant
on the cane. Physical examination
revealed a gap between two bony swellings on the anterior aspect of the knee. The
patient was unable to extend the knee with a flexion deformity
of 40 degrees. Radiographic
examination revealed that the patella had fractured and the two
pieces were separated by a gap
of 7 centimeters.
Due to the age of the
patient and the duration of the neglect, a patellectomy was
planned. However it was not
possible to bring the two fragments close enough clinically to
go ahead with the surgery
straight away. A significant quadriceps lag was apprehended. To overcome this potential
complication two Steinmann pins were passed transversely through the two
fragments of the patella. These were connected by a system of
threaded rods and plates. The
fragments were gradually brought together over a period of 10
days by applying compression
across the Steinmann pins with the help of the threaded rods. The final status was
maintained for one more week. After a total of 17 days a patellectomy was
carried out. During the surgery the cartilage of the patella was
found to be significantly
degenerated with significant tears in the expansions. A heavy
non absorbable suture was
placed through the margins of the patellar and quadriceps
tendons and through the medial
and lateral capsular expansions in a purse string manner. The suture was pulled taut
evaginating the tendons outside the joint. Supplemental
interrupted sutures to reinforce
the capsular repair and further appose the quadriceps and
patellar tendon ends were added.
Post operatively the patient was immobilized by a posterior splint for 3 weeks.
Range of motion exercises were instituted at 3 weeks. On a
followup at 9 months the patient
has no quadriceps lag and a 135 degree flexion. Ther was a 2.5 centimeter quadriceps
wasting.
 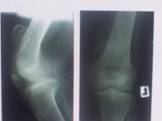
Fig 1
Fig 2
Fig 1:
Showing the
visible gap between the fracture fragments at the initiation of the application of the
compression fixation.
Fig 2: Radiographs
showing the large gap between the fracture fragments at the time of presentation.
 
Fig 3
Fig 4
Fig 3: Showing
the approximation of the fracture fragments after ten days of gradual compression.
Fig 4: Approximation
of the fragments is appreciable clinically as well.
Discussion:
The purpose of
reporting this case is to highlight the possibility of the use
of the Ilizarov method in preventing
quadriceps lag in patients of non union of patellar fractures
with large gaps between the
fracture fragments. 2.4% of patellar
fractures end in non union.
2
However non
union is well tolerated by patients with limited
or decreased functional demands on the knee. Non union of the patella with a large
gap between the fragments is a management challenge. The normal tensile forces across a
patella may reach 3000N and may increase to 6000N in atheletes.4
Daily activities
generate patellofemoral compressive forces greater than three
times the body weight, while
forces generated with stair climbing and deep squatting may
exceed seven times the body
weight.5
These forces act
on the proximal pole unopposed when the fracture is accompanied
by tears in the medial and lateral expansions. Preservation of
the medial and lateral
expansions along with anterior fascia lata and sharpey,s fibers
allows active extension of the
knee after patellar fracture. Unrestricted application of these forces, as in our case,
causes a progressive increase in the gap between the fragments
and a contracture of the
proximal quadriceps mechanism. In this situation the metabolism
of hyaline cartilage is
disturbed and synovial fluid functions are impaired. Hyaline
cartilage degenerates and
irreversible changes occur rapidly. Patella preservation
whenever possible is seen as a
preferable approach compared to other patellar resection
techniques, since a significant
loss of the extensor mechanism occurs when the patella is
partially or totally excised.6
However in certain
situations patellectomy is unavoidable. Advocates of
patellectomy enumerate shorter
immobilization, less complicated operative technique and an
earlier return to work as its
advantages.7,8
Patellectomy when
indicated is best accomplished by shelling out the fragments. Continuity between the
quadriceps and patellar tendons is provided either by imbrication or direct suture. The
tightness of repair is assessed by obtaining at least 90 degrees
of intraoperative knee
flexion before strain on the repair becomes noticeable.
Attaining a greater degree of
flexion, before the repair shows tension effects may increase
post operative extension
lag.
9
Reports of non union of
fractures of the patella
are rare.3,10,11
Satku et al
reported on the management of a large
gap non union of the patella. They used surgical mobilization
and tension band wiring.3
When shortening is such
that apposing the ends of the tendons is impossible, the
Stability is improved and a
practical range of knee motion is regained. However full
forceful extension may be
difficult to restore.Codavilla tendon lengthening technique may
be helpful, as described
by Scuderi.12
Our case demonstrates
that the application of the gradual compression to appose non union fragments of the
patella with a large gap, facilitates reconstruction of the quadriceps tendon,
eliminating quadriceps lag.
Reference:
-
Eric EJ.. Fractures
do joelho. In; Rockwood CAJ, Green DP, Bucholz RW. Fractures em adultos. 3rd
ed.
Philadelphia; Lippincott; 1991. p1729-44.
-
Nummi J; Fracture of
the patella; A clinical study of 707 patellar fractures. Ann.
Chir. Gynaecol. Fenn.,
60[Suppl 179]; 1-85, 1971.
-
Satku K, Kumar VP.
Surgical management of non union of neglected fractures of the patella. Injury 1991
Mar; 22[2]; 108-10.
-
Hubert HH, Hayes WC,
Stone JL, et al. force ratios in the quadriceps tendon and
ligamentum patellae. J
Orthop Res. 2; 49-54, 1984.
-
Rorabeck CH,
Bobechko WP. Acute dislocation of the patella with osteochondral fracture. A review of
eighteen cases. JBJS 58 A; 237-240, 1976.
-
Muller EJ, Wick M,
Muhr G. Patellectomy after trauma; Is there a correlation
between the timing and clinical
outcome. Unfallchirurg 2003; 106; 1016-9.
-
Brooke R. Fractured
patella; An analysis of 54 cases treated by excision. Br Med J 1946; 1; 231-233.
-
Levack B, Flannagan
JP, Hobbs S. Results of surgical treatment of patellar fracture. JBJS 67B; 476-419,
1985.
-
Eric E Johnson,
Rockwood and Greens Fractures in adults. 4th
Ed V2 p1968. Lippincott
Raven. Carriera DA, Fox
JA, Freedman KB, Bach BR Jr. Displaced non union patellar fracture following use
of a patellar tendon autograft for ACL reconstruction; case
report. J Knee Surg 2005 Apr;
18[2] 131-4.
-
Espinosa Morales
R, Escalante A. Gout presenting as a non union of a patellar fracture. J Rheumatol
1997 Jul; 24[7];
1421-2.
-
Scuderi C. Ruptures
of the quadriceps tendon; Study of twenty tendon ruptures. Am J Surg 95; 626, 1958.
|

