|
Abstract
External fixator in compound fractures with
exposed bone is well accepted and time tested. But in cases
where the bone is not exposed but internal fixation is not
possible external fixators have a role, which is not well
documented in the literature. The key to success is not to
expose the fracture site. For achieving closed reduction with
external fixator only a few options are available which are
either expensive or are very cumbersome. We herein describe a
versatile external fixator, which can be used to achieve closed
reduction. The fixator described over scores its counterparts
not only in terms of cost but also in terms of versatility and
stability .We recommend this fixator in cases where closed
intramedullary nailing for one reason or another is
inappropriate.
Keywords:
External fixator; closed reduction; versatile; inexpensive.
J.Orthopaedics 2007;4(1)e10
Introduction:
We still have a long way to go before the best treatment for the
fracture tibia can be stated with finality (Sir John Charnley).
Last decade has seen a major shift in the
principles of fracture fixation from mechanical to biological,
rigid to semi-rigid and from open to closed methods of fixation.
With the advent and popularisation of C-arm and availability of intramedullary interlocking nails, the above-mentioned
principles of closed, biological and semi-rigid fixation are
achieved. Intramedullary interlocking nails are used worldwide
for closed as well as open fractures of long bones. Yet the
problems are not fully solved. Some of the criticisms are
violating the medullary canal with a foreign body, technically
demanding, introduction of infection in potentially compound
fractures, intraoperative hazards of radiation and fat embolism,
bending and breakage of implant, tedious and sometimes difficult
removal of implant. Hence closed biological fixation by
intramedullary interlocking nailing has not answered all the
questions, and has made us to rethink about other methods of
achieving closed biological fixation.
Role of external fixators in compound fractures
with exposed bone is well accepted and time tested. Some of the
advantages of external fixator are it being a simple procedure,
which can be done quickly in a high-risk polytrauma patient, and
it provides with all the advantages of early fixation and
maintains good alignment and length of the bone with minimal
soft tissue damage. As the pins take purchase in the bone away
from the fracture site and do not interfere with the fracture
site it decreases the chance of ominous complication like
infection and also provides access to soft tissue management.
The damage to the perifocal tissue is minimal as there are very
few gripping elements in each fracture fragment. The method
allows for direct surveillance of the limb and wound status,
including wound healing, neurovascular status, viability of skin
flaps and tense muscle compartments. Associated treatment (e.g.
dressing change, skin grafting, bone grafting and irrigation) is
possible without disturbing the fracture alignment or fixation 1. In cases of fracture with head injury, which has
an extraordinary propensity for rapid consolidation, the
external fixator provides for stable and definitive reduction of
the fracture even during the first day with relative modest
surgical risk.
The conventional external fixator requires dissection
at the fracture site to get a good reduction thus increasing the
tissue trauma. Long back in 1952 J. R. Moore said I appeal-
keep the closed fracture closed, he had a great point in it,
now we all know. It will obviously be a great advantage if we
can get all the benefits of external fixation without exposing
the fracture site. Role of closed external fixator in closed
fracture is limited at present to comminuted metaphyseal
fractures where the principle of ligamentotaxis is used for
achieving closed reduction and alignment. Some of the existing
methods of achieving closed reduction by external fixator are by
using ring fixator with translation and rotation device in
Ilizarov system 2 and reposition device in Oganasean
system 3. They are really very cumbersome and
non-complaint. Although this has been achieved by an Orthofix,
but it is very expensive and has some limitations 4.
The design of the Orthofix imposes fixed minimum and maximum
distance between the clamps. Also the position and the direction
of the pin placement are fixed in relation to each other
allowing no flexibility to pin placement 4.
We are describing an external fixator, which has all
the advantages of external fixator with an added luxury of
obtaining closed reduction. It also allows late adjustment in
the reduction and above all can be used to give compression at
the fracture site. The surgeon has all the freedom for the pin
placement with respect to both, the distance between pins and
the plane in which pins are passed. Moreover it is not expensive
when compared to other external fixators used for closed
reduction. In a seriously injured patient with multiple
fractures and high risk for surgery it can even be applied in
the casualty without worrying about the quality of reduction,
which can be later improved under C-arm guidance or even in the
X-ray room.
Description of the device:
This is a unilateral external fixator system whose
central body and tubular rods are axially coupled by means of
ball and socket joints. On the basis of experienced gained by
using other fixators we set our self the following objectives
while designing this device:
-
Unilaterality
-
Axial
Controlled compression
-
Light weightArticularity in different planes
-
Simplicity of application
-
Simple instrumentation
-
Modularity in using for any site of any long bone in all age
groups
The device consists of:
Two rods (Fig. 1a) of unequal size at either ends connected to
each other by a central corrective assembly consisting of ball
and socket joints at both ends and a central compression and
distraction assembly. Each ball and socket joint has a working
angulatory capacity of about 30 degrees in all directions. This
theoretically makes the device to correct any angulation of the
extent of about 60 degree in any direction (Fig. 2). The central
distraction and compression assembly allows an axial movement of
nearly 2.5 cms (Fig. 3), enough not only to correct the usual
overriding or telescoping displacement at the fracture site but
also to mildly over-distract the fracture site prior to
correction of the angulation or translation at the fracture
site. Each of these three components two ball and socket joints
and one compression-distraction assembly are independently
locked by the hexagonal nuts (Fig. 1B [arrow]).
The design of the central corrective assembly like Orthofix
imposes a fixed minimum distance between two pins closest to the
fracture site, one each on either side of the fracture. But this
has been overcome in our system by providing an additional
supplementary Lambda rod (Fig. 1C), which serves two important
purposes. Firstly it allows the surgeon to introduce and
incorporate an additional pin closer to the fracture site
(proximal or distal to the fracture site) in a different plane
to enhance the stability of the fixation which is otherwise not
possible because of the fixed minimum distance between the two
innermost pins closer to the fracture site on either side of the
fracture site. Secondly, by virtue of being a supplementary
second rod with the shape of Greek word lambda (λ) , purchasing
a minimum of three pins (two pins closest to the fracture site
on either side of the fracture and the third pin placed in a
slightly different plane between the above mentioned pins either
proximal or distal to the fracture site) spanning the fracture
site it acts as a locking mechanism for the entire central
corrective assembly (Fig. 3 & 6), preventing loss of reduction
due to accidental loosening of locking hexagonal nuts of the
ball and socket joints and that of compression-distraction
assembly.

Fig 1.
Fig 2.
Fig 3.
Fig 4.
Fig 5.
Fig 6
 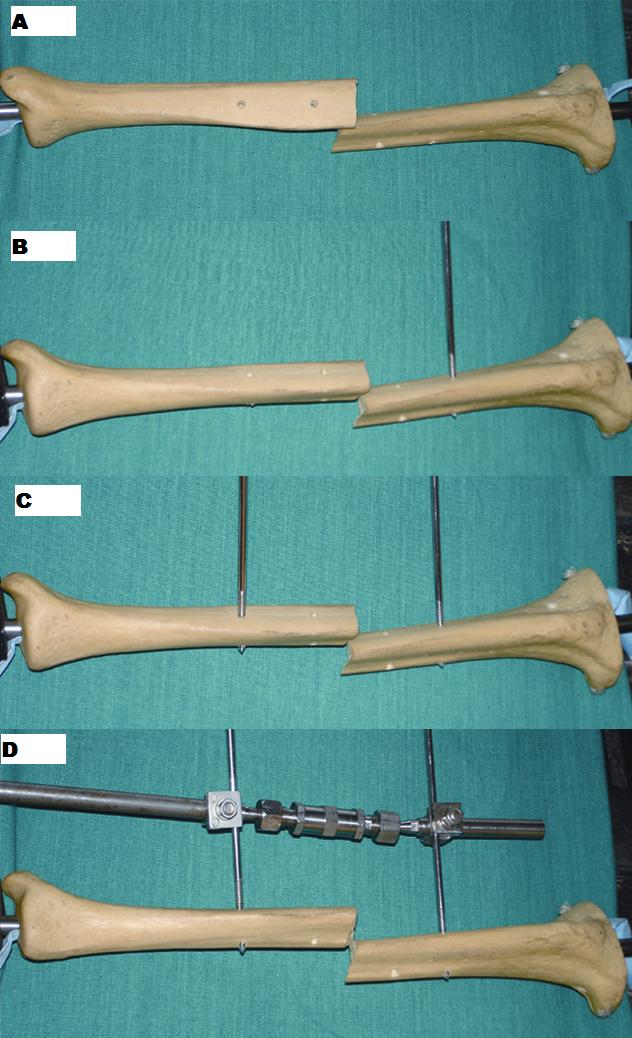
Figure 1: (A) Two rods of unequal size and central corrective
assembly.
(B) Rods and central corrective assembly
assembled.
(C) Lambda rod
Figure 2: Model showing the amount of translation and
angulations which can be corrected by described fixator.
Figure 3: Model showing the amount of compression and
distraction which can be achieved be the assembly.
Figure 4: (A-D) Steps of fixator application (Refer text for
details).
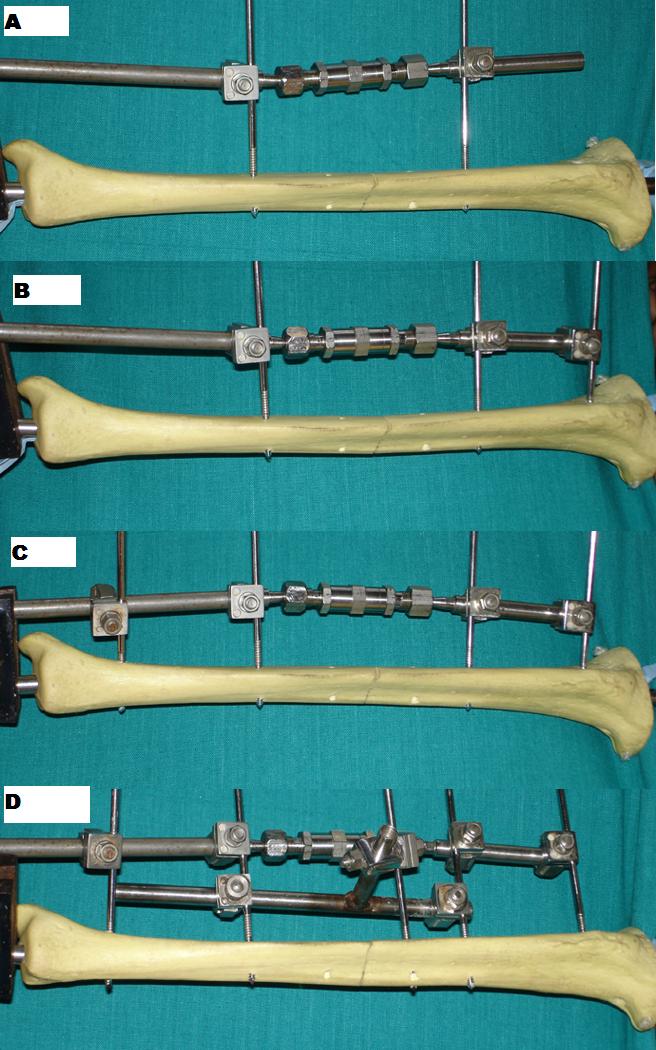
Figure 5: (A-D) Steps of fixator application (Refer text for
details).
Figure 6: Clinical picture showing the fixator in place for one
of the cases.

Indications:
All the cases where intramedullary nailing of the tibia in not
possible and the surgeon wants to have all the advantages of
closed fixation:
-
Degloving injury with fracture bone not exposed
-
Impending compartment syndromePotentially compound fractures (wound not communicating with the
fracture site)
-
Unhealthy skin over the nail entry site
-
A polytrauma patient who is high risk for long anaesthesia it
will decrease the duration of surgery.
Methods
In order to make best use of fixator, with least exposure to the
radiation we recommend the following technique for achieving
closed reduction of the fracture shaft of the tibia:
Patient is given general or spinal anaesthesia and placed on a
table compatible with C-arm. Under aseptic precautions, two
Schanz pins are placed one on either side of the fracture site
preferably over the antero-medial surface of the tibia (Fig. 4
A-C). One of these pins can be closer to the fracture site than
the other but the distance between the two pins should be at
least 1 cm more than the minimum fixed distance determined by
the length of the central corrective assembly (in our system
this distance is 10 cms) (Fig. 4D) Now an attempt of closed
reduction is performed with the help of C-arm (Fig. 5A). The
pins on the proximal and distal fragments can be used as
joysticks to gently manoeuvre the fragments for closed
reduction. Once a reasonable closed reduction is achieved the
fixator is applied purchasing the two pins using standard
universal clamps with the rods of the fixator, whose two ball
and socket joints are in neutral position and the central
corrective assembly opened midway (with a provision to compress
or distract 1.25 cm on each side). Now with the fracture
reduction maintained, the fixator is locked by tightening the
hexagonal nuts (Fig. 5B). Now the third and fourth Schanz pins
are introduced in the proximal and distal metaphyseal region in
the site and direction suitable for the particular case (Fig.
5C). Once all the four Schanz pins are placed, the fine tuning
of the closed reduction can be obtained by loosening the nuts of
both the ball and socket joints. Compression or distraction can
be achieved without loosening of the
nuts
of the ball and socket
joint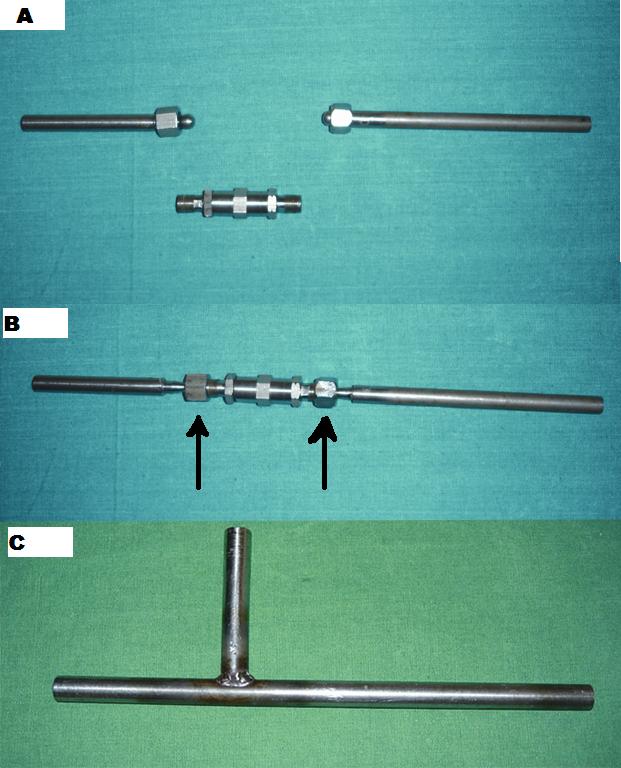 s.
Additional purchase of the skeleton using a Lambda
rod is now achieved by introducing a separate Schanz pin closer to the
fracture site proximal or distal to the fracture site (Fig. 5D).
This Lambda rod will take purchase at this eccentric pin and at
least two pins, one on either side of the fracture site. This
Lambda rod thus locks the central corrective assembly and also
enhances the mechanical fixation by virtue of being between the
skeleton and the central corrective assembly of the fixator
(Fig. 6). s.
Additional purchase of the skeleton using a Lambda
rod is now achieved by introducing a separate Schanz pin closer to the
fracture site proximal or distal to the fracture site (Fig. 5D).
This Lambda rod will take purchase at this eccentric pin and at
least two pins, one on either side of the fracture site. This
Lambda rod thus locks the central corrective assembly and also
enhances the mechanical fixation by virtue of being between the
skeleton and the central corrective assembly of the fixator
(Fig. 6).
Alternatively this eccentric Schanz pin for the Lambda rod may
be introduced following the introduction of first two pins and
before the application of the fixator. This may be preferred
because it will be difficult to pass the eccentric pin in the
diaphyseal cortical bone with the universal clamp used as drill
guide without disturbing the fracture reduction. For mechanical
reasons this eccentric Schanz pin is introduced on that side
(proximal or distal) of the fracture site which has a greater
distance between the fracture site and the Schanz pin closest to
the fracture site. Similar procedure can be used for the
metaphyseal fractures by using a transverse metaphyseal
fractures by using a transverse metaphyseal clamp on the smaller
metaphyseal fragment.
Though we are not claiming for any originality of the method or
the principle, to the best of our knowledge we have not come
across any external fixator being used for closed reduction
incorporation tubular system and universal clamps.
Contraindications:
We do not recommend this
external fixator in cases of segmental fractures, fractures with
bone loss and metaphyseal fractures with intra-articular
extension.
Reference:
-
Kovafix External fixator
system. Surgical technique instruction manual. The Coimbatore
Surgical Pvt. Ltd., BB Street, Coimbatore India.
-
De Bastiani G, Aldegheri
R, Brenzi Brivo L. Dynamic axial external fixation. Clinical
Orthopaedics, India; 1990; Vol.5: 160-177
-
Woods GW. General
principles of fracture treatment. In Campbells Operative
Orthopaedic. 9th ed. Cannale TS. Mosby. 1998: 2669-2723.
-
Galyakhovsky Vl, Frankel
VH. Operative Manual of Ilizarov Technique. 1st Indian ed.
Peter L Ferrace. Jaypee Brothers. 1994.
|

