|
*A. Elmrini, +S.
Boujraf, *O. Agoumi, *A. Daoudi, #A. Afifi, *F. Boutayeb, *A.
Marzouki
*Department of Orthopedic and Traumatic Surgery, University
Hospital Hassan II, Fez.
+Department of Biophysics and MRI Methods, Faculty of Medicine and
Pharmacy, University of Fez
#Department of Pediatric Surgery, University Hospital Hassan II,
Fez.
Address for Correspondence
Dr. A. Elmrini,
Department of Orthopedic and Traumatic Surgery,
Al Ghassani Hospital, University Hospital Hassan II, Fez 30000.
Morocco.
Phone: +212 61 107 741,
Fax: 00 212 55 619 321
E-mail: traumajid@yahoo.fr |
|
Abstract
We report one case of a traumatic circumscribed ossifying
myositis developed from the vastus medialis muscles, in an 18
years old male. Six months after surgical treatment, we obtained
results consisting of an excellent functional outcome without
recurrence.
Key words: ossifying myositis ; Vastus Medialis
J.Orthopaedics 2006;3(3)e8
Introduction:
The confined ossifying myositis is a pseudo
tumoral affection. It consisted of none neoplastic and
heterotopic site of bone or cartilage. This develops in soft
tissues.
We report a case of ossifying myositis in the
vastus medialis muscles of the thigh, which adhered to the
member in the pediculosis femora. The surgical resection was
complete.
Case Report:
The patient R. M of 18 year-old, without
particular antecedent. He presented with pain of 6 months at the
level of the medial side of the thigh; with a swelling at the
same level, which has had a gradual increasing size. No change
of the general status was noticed, and no infectious signs were
present.

The clinical examination revealed a hard
swelling of 4 centimeters diameter that has not inflammatory
character, but sensitive squeeze; it was adhering to the deep
structures but movable with regard to the superficial plane.
There was neither the cutaneous modification, nor
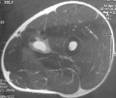
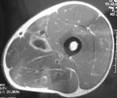
vascular-nervous disorder. The femoral radiography showed a
fan-shaped calcification. The MRI showed a hyper signal mass of
the vastus medialis muscle,(fig. 1). From these two examinations
we concluded ossifying myositis. The surgical process consisted
of, dissecting the tumor and the femoral artery; this last one
was whitish, rigid and calcified by lay which required the
resection its entirety (fig.2). The histological study confirmed
the diagnosis of ossifying myositis. The evolvement after a
recession in period of 6 months did not show any recurrence.
Discussion :
The term of confined ossifying myositis or
pseudo tumor denote a clinical entity characterized by
histological lesions consisting of muscular and conjunctival
progressive ossifications [1]. It is a rare affection of the
childhood [2, 3]. Only 25 cases were assessed in the literature
[2]. Sometimes an acquiescent ground is found such as
paraplegia, burn, tetanus [4]. This occurs in young adults, and
in equal way in both sexes [1, 5, 6]. The diagnosis is approved
at the stage of calcification [3, 6]. It is suspected of a tumor
of hard consistency in the lower limb; it is evoked in the
radiography, given that the existence of a clear zone separating
the adjacent bone lesion with cortical integrity. The periosteal
reaction could lead to confusion. In contrast, Battistelli et al
[7], Brofen et al [2], Crouzet et al [8], Goldman [9], Gougeon
et al [10], underline the complexity to diagnose, especially in
the early stage where the pathology simulate malignant lesion.
The diagnosis is based on clinical, ultrasound, CT-scan, MRI and
anatomic-pathology examination. The CT-scan shows compatible
hyper-dense sectors with beginning calcifications, it allows
also pointing the integrity of the primary cortical bone. The
MRI allows checking the integrity of the neighborhood structures
including muscle, vascular-nervous pedicle; it could eliminate
in certain cases the diagnosis of tumor. The injection of
gadolinium seems to be very useful to judge the extension and
the heterogeneity of the lesion in T1 images [4, 11]. The
histological exam confirms the diagnosis of ossifying myositis,
this shows typical lesion formed in three concentric layers: the
centre constituted of undifferentiated mesenchymal cells,
surrounded by intermediate zone that is affluent of osteoid,
limited by a line of osteoblast. The final layer is composed of
mature bone which encircles the lesion; where the muscular
fibers and the soft tissues are intact [6-8, 10-12].
At the calcification stage, the significant
ossification could let to critical situation of a chondrosarcoma
or an osteosarcoma of soft parts. Mostly, the clinical context
and the appropriate para-clinical examinations allow eliminate
any doubt. The disease of Münchmeyer shows the same histological
characteristics of the ossifying myositis, it is different by
its hereditary character, the accompanying osseous alteration
(absence or shortening of a phalanx of the big toe, of the
thumb), and it has critical prognostic [1]. The prognostic is
excellent. Indeed, recurrence is exceptional and always followed
by cure after re-intervention [6, 7, 12]. 12 months after
surgery, our patient did not show any recurrence. Masquelet [5]
and Serratrice [1] suggest a medical treatment by
anti-inflammatory drugs and diphosphonates. This medical
treatment would minimize the risk of ossification appearance.
Brofen [2] also finds that the ossifying myositis has a
spontaneous favorable evolution, he recommends the ablation only
in two cases: severe pains and\or important and extended
functional impairment, and in case of diagnostic doubt.
Conclusion
None traumatic ossifying myositis presents an
excellent prognostic. However, it is difficult to diagnose with
certainty, especially in the late stages, this to not
underestimate a malign tumor. In spite of the contribution of
the CT-scan and MRI that is incontestable; the histology
examination is still establishing the diagnosis.
Reference :
- Serratrice G. Pathologie médicale des muscles striés du
squelette. Encycl Méd Chir (Paris-France), Appareil Locomoteur,
15151A 20, 10-1988, 12 p.
- Brofen. C, Touzet PH, Peuchmor M et al. Myosite ossifiante
circonscrite non traumatique chez l'enfant.
Revue de la littérature: à propos d'un cas simulant une tumeur
maligne. Rev Chir Orthop, 1993: 229-234.
- Diaine B, Kurzenne JY, Hofman P et al. Myosite ossifiante
circonscrite pseudo-tumorale de la paroi thoracique.
Apport respectif de l'échographie, de la
tomodensitométrie et de l'I.R.M. Radiol, 1993: 87-90.
- Bouchardy L, Garcia J. Apport de l'imagerie par résonance
magnétique (I.R.M) dans le diagnostic de la myosite ossifiante
circonscrite (M.O.C). Radiol, 1994: 101-110.
- Masquelet AC. Ossifications et tumeurs
musculaires, In: Pathologie chirurgicale, tome 3, Nordin JY,
Masquelet AC. Masson, Paris, 1992.
- Ogilvie-Harris DJ, Hons ChB. Pseudomalignant myositis
ossificans: heterotopic new-bone formation without a history
of trauma. J Bone Joint Surg, 1980: 1274-1283.
- Batistelli JM, Pauline-Balas D: Myosite ossifiante
circonscrite non traumatique à localisation cervicale. Apport
de la tomodensitométrie. Ann Péd, 1988: 59-63.
- Crouzet J, Chomette G. Myosite ossifiante circonscrite non
traumatique. Difficultés diagnostiques. À propos d'une
observation. Rev Rhum, 1983: 213-216.
- Goldman AB. Myositis ossificans circumscripta: a benign
lesion with a malignant differential diagnosis. A.J.R.,
1976:32-40.
- Gougeon J, Dousset M. La myosite ossifiante circonscrite
non traumatique. Observation anatomo-clinique d'un cas et
revue générale. Rev Rhum, 1970: 367-373.
- Mathonnet M, Longis B, Moulies D. Myosite ossifiante
circonscrite non traumatique. Problème diagnostique. Ann
Orthop Ouest, 1992: 91-94.
- Anglejean G, Perez C. Myosites ossifiantes circonscrites.
Actualités rhumatologiques, 1984: 153-159.
|

