|
Abstract
Carpal tunnel release has
become one of the most frequent and successful operative
procedures performed on the hand. However, complications and
treatment failures have been shown to occur in 3% to 19% in
large clinical series, needing re-exploration in up to 12% of
open carpal tunnel release 1. Common causes of unrelieved
symptoms or recurrence are diverse and include incomplete
release of the transverse carpal ligament, reformation of the
flexor retinaculum, postoperative adhesions, fibrous
proliferation, scarring within carpal tunnel, recurrent
inflammatory flexor tenosynovitis, entrapment of the palmar
cutaneous branch, laceration or neuroma of median nerve or
palmar cutaneous branch, incorrect diagnosis, double crush
syndrome, etc 2. Of these the most common pathologic finding was
epineural scarring at the site of decompression surrounding the
nerve 3. When this occurs, multiple surgical procedures have
been advocated to diminish adherence of the median nerve,
including reincision of the transverse carpal ligament, scar
debridement, epineurolysis, internal neurolysis, placement of
local muscle flaps or fat pads over heavily scarred areas, and
application of barrier material to prevent recurrence of
adhesions 2.
We present an alternative
method to treat this complication. This method of treatment
called Vein wrapping constitutes a simple surgical technique
that causes minimal complications in the donor area. In
addition, the donor vein is readily available and harvesting is
easy.
J.Orthopaedics 2006;3(2)e9
Material and Methods :
We treated two female
patients with recurrent compressive neuropathy of the median
nerve by means vein wrapping. Our first patient was a 42
year-old woman diagnosed of carpal tunnel syndrome of her right
hand 2 years before. She has been operated previously twice but
symptoms reappeared each time after few months of clinical
improvement. She had diabetes mellitus type 1 and penicillin
allergy. The second patient was a 51 year-old woman operated
in other centre of carpal tunnel syndrome of her right hand 1
year before. Following carpal tunnel release she was free of
symptoms for 2 months but the numbness gradually recurred. She
suffered from cardiac pathology, hypercalcemia, chronic venous
insufficiency, cervix cancer resection and she also had
penicillin allergy.
The average follow-up
period was 12 months. Each patient had both subjective and
objective evaluation. For the subjective evaluation the patient
was given an identical questionnaire both before and after
surgery that asked about pain, numbness, and overall
satisfaction. Patients were asked to rate their level of pain on
a scale of 10 and to state whether their preoperative numbness
had improved after surgery. They also were asked whether they
were satisfied with the outcome. The objective evaluation
included the measurement of 2-point discrimination and grip
strength by means a Jamar dynamometer. No electrodiagnostic
studies were performed after surgery.
Surgical Technique
:
Under general anaesthesia
the ipsilateral or contralateral lower extremity is used for
haversting the internal saphenous vein. A longitudinal incision
is made anterior to the medial malleolus (Fig. 1). However the
vein graft can be haversted by means a vein stripper to minimize
the length of the incision and the morbidity of the donor site.
The required length of the vein is 3 to 4 times the scarred
length of the nerve (aprox 25 to 30 cm). The remaining internal
saphenous vein is ligated both proximally and distally before
the excision of the graft. With the help of sutures or skin
hooks the graft is held straight and is incised longitudinally,
using a pair of sharp scissors, to form a rectangle (Fig 2).
  
Figure 1. Preparation of the
saphenous vein graft. A) Skin incision. B)
Visualization of the vein. C) Dissection of the vein.
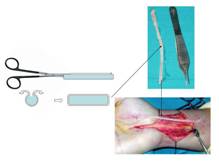
Figure 2. Preparation of the vein
graft.
With respect to the wrist,
we performed the standard surgical approach for carpal tunnel
release, but slightly extended proximally and distally, to
expose the median nerve in an unscarred environment. In both
cases a great fibrous proliferation was found constricting the
nerve proximally just to the palmar cutaneous branche, and
distally just at the level of the distal carpal tunnel in which
the nerve divides into lateral and medial portions under the
palmar aponeurosis and the superficial palmar arch (Fig. 3).
The involved nerve is first decompressed and separated from all
the scarred soft tissues. After then, the vein intima was placed
next to the nerve, and circumferential wrapping distal to
proximal is performed.
 Figure
3. Scar tissue around the median nerve. Figure
3. Scar tissue around the median nerve.
One end of the vein graft is tacked distal
to the scarred portion of the nerve on a tissue that is not
mobile, generally in one of the lips of the opened transverse
carpal ligament (Fig. 4), while the other end of the vein graft
is tacked proximal to the scarred segment of the nerve on
unscarred tissue, generally immediately
distal to the exit of the palmar
cutaneous branch (Fig. 5).
 Figure
4. Distal attachment of the graft
in one of the lips of the opened TCL. Figure
4. Distal attachment of the graft
in one of the lips of the opened TCL.
The vein-to-vein junctures were sutured
carefully with 6/0 non-absorbable monofilament.
 Figure
5. Vein graft wrapping completed. Observe that the
sapheonus vein covers the entire portion of the nerve. Figure
5. Vein graft wrapping completed. Observe that the
sapheonus vein covers the entire portion of the nerve.
During the wrapping procedure, care is
taken to avoid nerve traction or suturing of the vein to the
median nerve (Fig. 6).
 Figure
6. A soft tissue-elevator could be
passed easily between the wrapping vein. Figure
6. A soft tissue-elevator could be
passed easily between the wrapping vein.
The skin was closed with
5/0 monofilament and wrist was immobilized in 20 degrees of
neutral position with antebrachial splint for 2 weeks. Active
and passive motion exercises are started immediately after the
splint is removed.
Results :
Six months after surgery, all patients
reported a reduction in pain and the sensory disturbances
secondary to the compression of the median nerve. On a scale of
10, both patients rated their pain between 2 and 3; their
preoperative pain had been rated between 8 and 9. Sensation
improved in both patients. Two-point discrimination improved
from 10 and 13 respectively before surgery to 5 and 7 after
surgery. Grip strength increased from 15 and 20 Kg respectively
before surgery to 22 and 30 after surgery. However, the patients
reported discomfort at the saphenous vein donor site that
resolved at approximately 4 weeks after the procedure. There are
no infection case.
Discussion :
Despite a high rate of
success following an initial carpal tunnel release, there are
subsets of patients who report persistent or recurrent symptoms
and needed secondary carpal tunnel surgery.
Although some risk factors which may also
contribute to the need for secondary surgery as diabetes
mellitus or hypertension associated with medical therapy with
b-blockers 4, the main reason for failure is the scar tissue
that develops at the site of decompression surrounding the
nerve. The risk factors for development fibrous proliferation
following carpal tunnel release remain unknown, but poor
hemostasis and hematoma formation, prolonged postoperative
immobilization, inadequate range-of motion exercises and therapy
have been implicated. In these circumstances, revision carpal
tunnel release followed by internal neurolysis has a high rate
of persistent symptoms and poor results 5. For this reason
numerous methods of operative treatment for recurrent entrapment
neuropathy have been described, fundamentally local muscle flaps
or fat pads over heavily scarred areas, and application of
barrier material to prevent recurrence of adhesions. Therefore,
small local flaps, such as the abductor digiti minimi, the
palmaris brevis, and the pronator qadratus, also have been used
6,7,8,9,10,11,12,13,14,15,16. However, the dissection of these
flaps is not always ease, because vascular pedicles have limited
mobility, nerve coverage is sometimes inadequate, and skin
closure problems may occur.
The primary indication for a vein wrap
following the neurolysis is the presence of significant
epineural scarring that can prevent nerve gliding. The
technique of vein wrapping was first described by Gould 17 for
treatment of painful neuroma in-continuity, but was Masear et
al. 18 which first reported the successful use of a vein graft
for recurrent symptoms secondary to scarring of the nerve. Six
years after, Masear and Colgin 19 to report clinical results
with the use of a vein wrapping for recurrent median nerve
compression. Koman et al. 20 used allograft umbilical vein for
median nerve dysfunction with good results and Soteranos et al.
21,22 reported significant pain relief in patients with
recurrent carpal tunnel syndrome after treatment with vein
wrapping.
Our results were
comparable with others series in the sense that the autogenous
vein wrapping technique is effective in the treatment of a
compression neuropathy secondary to scar. However, the exact
mechanism of its effect remains uncertain. In this aspect, in an
experimental study Xu et al. 23,24 used the
femoral vein to wrap the sciatic nerve of rats and found that no
scar tissue developed between the epineurium of the wrapped
sciatic nerve and the intimal surface of the vein. Vardakas et
al. 25 report a case which provides clinical intraoperative
evidence in human of the lack of scar tissue between the intimal
surface of the vein and the epineurium of ulnar nerve wrapped
two years before for recalcitrant cubital tunnel syndrome.
In conclusion, the use of
autogenous vein wrapping technique is a good alternative for
treatment of recurrent median neuropathy secondary to scarring
of the nerve.
Reference:
-
Botte MJ, von Schroeder
HP, Abrams RA, Gellman H. Recurrent carpal tunnel
syndrome. Hand Clin 1996; 12: 731-43.
-
Tung THH, Mackinnon SE.
Secondary carpal tunnel surgery. Plast Reconstr Surg 2001;
107: 1830-43.
-
Hunter JM. Recurrent
carpal tunnel syndrome, epineural fibrous fixation, and
traction neuropathy. Hand Clin 1991; 7: 491-504.
-
Schreiber JE, Foran MP,
Schreiber DJ, Wilgis FS. Common risk
factors seen in secondary carpal tunnel surgery. Ann Plast
Surg 2005; 55: 262-5.
-
Rhoades CE, Mowery CA,
Gelberman RH. Results of internal neurolysis of the median
nerve for severe carpal-tunel syndrome. J Bone Joint Surg
1985; 67 A: 253-6.
-
Plancher KD, Idler RS,
Lourie GM, Strickland JW. Recalcitrant carpal tunnel. The
hypothenar fat pad flap. Hand Clin 1996; 12: 337-49.
-
Reisman NR, Dellon AL.
The abductor digiti minimi muscle flap: A salvage technique
for palmar wrist pain. Plast Reconstr Surg 1983; 72: 859-63.
-
Koncilia H, Kuzbari R,
Worseg A, Tschabitscher M, Holle J. The lumbrical muscle flap:
Anatomic study and clinical application. J Hand Surg 1998; 23:
111
-
Tham SKY, Ireland DC,
Riccio M, Morrison WA. Reverse radial artery fascial flap: A
treatment for the chronically scarred median nerve in
recurrent carpal tunnel syndrome. J Hand Surg 1996; 21 A: 849
-
Wintsch K, Helaly P.
Free flap of gliding tissue. J Reconstr Microsurg 1986; 2: 143
-
Rose EH, Norris MS,
Kowalski TA, et al. Palmaris brevis
turnover flap as an adjunct to internal neurolysis of the
chronically scarred median nerve in recurrent carpal tunnel
syndrome. J Hand Surg 1991; 16A:
191201.
-
Dellon AL, Mackinnon SE.
The pronator quadratus muscle flap. J
Hand Surg 1984; 9A: 423427.
-
Jones, N. F., Shaw, W.
W., and Katz, R. G. Circumferential wrapping of a flap around
a scarred peripheral nerve for salvage of end-stage traction
neuritis. J. Hand Surg 1997; 22 A: 527
-
Spokevicius, S., and
Kleinert, H. The abductor digiti minimi flap: Its use in
revision carpal tunnel surgery. Hand
Clin 1996; 12: 351
-
Rose, E. H. The use of
the palmaris brevis flap in recurrent carpal tunnel syndrome.
Hand Clin 1996; 12: 389.
-
de Smet L, de Nayer W, Van
de Meulebroucke B, et al. Pronator
quadratus muscle flap for the treatment of neuroma in
continuity at the wrist. Acta Orthop Belg 1997; 63: 110112.
-
Gould JS. Treatment of
the painful injured nerve in-continuity. In: Gelberman RH, ed.
Operative nerve repair and reconstruction. Philadelphia: JB
Lippincott, 1991: 1541-9.
-
Masear VR, Tullos JR, St
Mary E, Mayer RD. Venous wrapping of nerve to prevent
scarring. J Hand Surg 1990; 15 A: 817-8.
-
Masear VR, Colgin S.
Treatment of epineural scarring with allograft vein wrapping.
Hand Clin 1996; 12: 773-9.
-
Koman AL, Neal B,
Santichen J. Management of the postoperative painful median
nerve at the wrist. Orthop Trans 1995; 18: 765
-
Soteranos DG,
Giannakopoulos PN, Mitsionis GI, Xu J, Herndon JH. Vein-graft
wrapping for the treatment of recurrent compression of the
median nerve. Microsurgery 1995; 16: 752-6.
-
Soteranos DG, Xu J.
Vein-wrapping for the treatment of recurrent carpal tunnel
syndrome. Tech Hand Upper Extremity Surg 1997; 1: 35-40.
-
Xu J, Soteranos
DG,Moller AR, Jacobsohn J, Tomaino MM, Fisher KJ, Herndon JH.
Nerve wrapping with vein grafts in a rat model: a safe
technique for the treatment of recurrent chronic compressive
neuropathy. J Reconstr Microsurg 1998; 14: 323-30.
-
Xu J, Varatimidis SE,
Fisher KJ, Tomaino MM, Soteranos DG. The effect of wrapping
scarred nerves with autogenous vein graft to treat recurrent
chronic nerve compression. J hand Surg 2000; 25 A: 93-103.
-
Vardakas DG, Varatimidis
SE, Soteranos DG. Findings of exploration of a vein-wrapped
ulnar nerve: Report of a case. J Hand Surg 2001; 26 A: 60-3.
|

