|
ABSTRACT
We
reviewed 14 patients who underwent Oxford Unicompartmental Knee
replacement and compared them with 14 patients with Anteromedial
compartment Osteoarthritis who underwent Total Knee Replacement.
Follow up period ranged from 8 months to 2years
9months(Mean-1year 3months). Outcome was assessed according to
Oxford knee score, pain score and range of motion. No
complications occurred. Functional results were the same in the
two groups during this period.
We conclude that there is
no difference in short-term results between Oxford
Unicompartmental Arthroplasty and Total Knee replacement for
Anteromedial Osteoarthritis of Knee. (Keywords- Anteromedial
Osteoarthritis, Oxford Unicompartmental Knee replacement, Total
Knee replacement, Outcome, Short-term review)
J.Orthopaedics 2005;2(2)e3
Introduction
Surgical
management of Osteoarthritis confined to the medial compartment
of the knee remains a matter of controversy (1). Few studies
have compared the outcome of Unicompartmenal Arthroplasty with
Total Knee replacement (1), with the same pathology (Anteromedial
Osteoarthritis).
Unicompartmenal Arthroplasty for selected cases of OA knee is
less invasive, preserving cruciate ligaments, provides better
range of motion and more physiological functions (2)(3).
The
operation has a lower morbidity, blood transfusion is not
required and the implant is cheaper.First Oxford
Unicompartmental replacement was performed in 1982(2), which is
the natural evolution of the original Meniscal arthroplasty used
in 1976(4).
If
performed early in the disease process, the operation can arrest
the progress of arthritis to the other compartments and provide
long-term relief in symptoms (2,13).
The latest Phase 3 OXFORD
KNEE is based on the clinical success of its predecessors, which
achieved 98 % survival of 10 years with average wear of
0.03mm/year (2,5). Continuous upgrading of the design and strict
selection criteria have started to give good results in selected
cases. (9,11)
Criteria for
Oxford Knee Replacement (2)
1.Both cruciate
ligaments must be intact, as stability of the prosthesis depends
on the intact cruciate mechanism.
2.Lateral compartment
should be well preserved with an intact meniscus and full
thickness articular cartilage, best demonstrated by AP x-ray
with joint in valgus stress.
3.Superficial
fibrillation, marginal osteophyte and localised erosions on the
medial margin of lateral condyle are not contraindications.
4.Malalignment of limb
should be passively correctable to neutral and not beyond.
5.Flexion deformity
should be less than 15 degree and further flexion up to 110
present on EUA.
6.Patello Femoral OA is
not a contraindication. In more than 500 cases by Munaj et al
no knee was revised for Patello-Femoral problems.
Contraindications:
1. Inflammatory arthritis
2. Lateral compartment OA.
Patients and
method
We had
28 patients in our study.15 were men, 13 women. Age was between
52 to 84 years (Mean-71 years). Follow-up period ranged from 8
months to 2years 9months. (Mean-1 year 3 months)
Selection of patients:
Between 1998 and 2000, Oxford Knee
replacement for Medial compartment Osteoarthritis was performed
in 18 patients by the senior author in Inverclyde Royal Hospital
which is a District General hospital. 14 patients were
available for follow-up in this group.
We
obtained X-rays and case notes of patients who underwent Total
Knee Replacement during the same period by two different firms
in the same hospital, who did not use the unicompartmental knee
replacement at the time of the study. The senior author
individually reviewed every X-ray. We selected the patients who
had Medial compartment Osteoarthritis whom would have been
considered for an Oxford Medial Unicompartmental Arthroplasty by
the senior author according to the radiological criteria,
(2,7,15). The total number in this group was 14. Further
confirmation was made after reviewing the case notes to confirm
the operative findings correlated with the radiological
findings.
Operative technique:
The senior author performed the
Oxford knee replacements. Medial minimal incision technique was
used in majority of the patients. Intra operative findings were
recorded and minor erosions in the lateral femoral condyle and
patello-femoral joints were ignored. Phase 3 components were
used. Palacos cement was used in both groups.
Two
different consultants carried out the Total Knee Replacements.
Midline incision was used, medial Para patellar approach for
Arthrotomy. Kinemax (Stryker-Howmedica) prosthesis was used in
all 14 patients. Hospital stay in both groups averaged between
5-7 days.
Review of patients:
All 28 patients were contacted by
post and reviewed individually in a special clinic arranged
exclusively for this study. Patients were first seen by a
Specialist nurse and the Oxford scores and Pain scores were
recorded, further reviewed by the first author for examination.
We decided to use the Oxford scoring and the pain score alone
because these were the only pre-op scores recorded in all
patients. Of the 4 patients not available for follow up 2 had
moved out of the area, 1 patient had a total knee replacement on
the opposite side and was excluded from the study.1 patient was
too frail and declined to attend the clinic.
Data
analysis:
Data was analysed using Microsoft
Excel, Independent t tests and Paired t tests.
Results
Of the
28 patients reviewed in the clinic all except 1 patient
(post-op- pain score 6/10) had excellent pain relief following
the procedures.
Mean
pre-op pain score- Oxford-8.71, TKR-9.43, p=0.082, no
significant difference.
Mean
post-op pain score-Oxford-1.43, TKR-1.86, p=0.364, no
significant difference.
The mean
range of movement in the Oxford knee group was 3-110 degrees
(Range of flexion-95-125), TKR was 2.5-105 degrees (Range of
flexion-70-125). The one patient with persistent pain had a good
range of movement and function, an obvious cause was not found
so far.
Oxford scores:
We
assessed the knee functional scores with the validated Oxford
knee scoring system (1,16). We are aware of the controversies
using this scoring system. We still think it is a good
reflection of the patient perception of function.
Mean
pre-op for Oxford 42.25, TKR-47.50,p=0.262,no significant
difference.
Mean
post-op for Oxford- 20.36, TKR-23.71, p=0.292 no significant
difference.
Radiographic assessment:
No
significant loosening was seen in either tibial or femoral
components in all the patients. So far none have had revision
surgery.
4
patients were not available for follow-up in the Oxford Group
.We did not receive any information from the General
Practitioner about the current status of these 2 patients who
have moved out of the area. We know that the remaining 2
patients had no problems with their knee through telephonic
conversation.
Results of the independent and paired t-tests:
Independent t-tests
Age by sex Mean age of females =
71; males = 72 \no significant diff p=0.672
Age by
type of knee replacement Mean age of OKR patients = 71; TKR =
71\no significant difference p=0.981
Pre-pain
by type of knee replacement - Mean pre-pain score of OKR
patients = 8.71; TKR = 9.43\no significant difference p=0.082
Post-pain by type of knee replacement - Mean post-pain score of
OKR patients = 1.43; TKR = 1.86\no significant difference
p=0.364
Oxford
pre-pain by type of knee replacement - Mean pain score of OKR
patients = 42.25; TKR = 47.50\no significant difference p=0.262
Oxford
post-pain by type of knee replacement - Mean pain score of OKR
patients = 20.36; TKR = 23.71\no significant difference
p=0.292
Paired t-test
Pre -0p pain compared with
Post-Op pain
All
patients mean pre-pain score = 9.07; mean post score = 1.64 \
significant diff p=0.000
OKR
patients mean pre-pain score = 8.71; mean post score = 1.43\
significant diff p=0.000
TKR
patients mean pre-pain score = 9.43; mean post score = 1.86\
significant diff p=0.000
Oxford
pre pain score compared with oxford post pain
All
patients mean pre-pain score = 44.5; mean post score = 21.14 \
significant diff p=0.000
OKR
patients mean pre-pain score = 42.25; mean post score = 20.88\
significant diff p=0.000
TKR patients mean
pre-pain score = 47.5; mean post score = 21.55\ significant diff
p=0.001
Discussion & Conclusions
There
are very few comparative studies of Uni-compartment knee
replacements compared with total knee replacements in the
literature. Newman et al (10) reported results on prospective
randomised study of 110 knees comparing Uni-compartmental
replacements and total knee replacements, without any
significance between the groups. They used the St George sleg
knee.
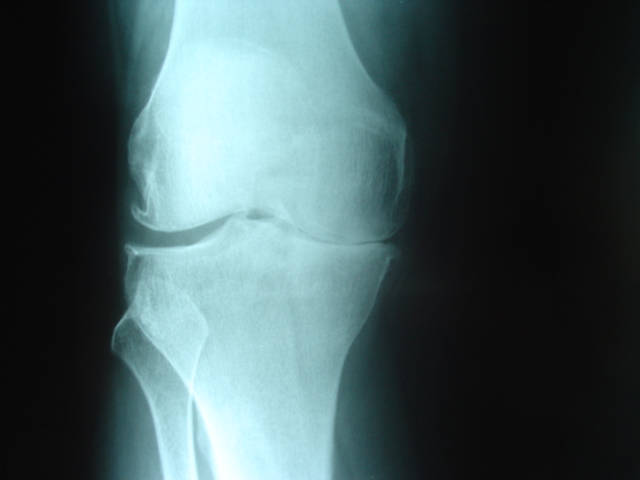
Figure 1A. Pre op AP xray of knee
with Anteromedial Osteoarthritis
There was a small increased range of motion in the Uni-compartmental
group as expected. Weale et al (1) showed that neither pain nor
function al outcomes were significantly different, although the
Uni-compartmental group were better able to climb stairs.
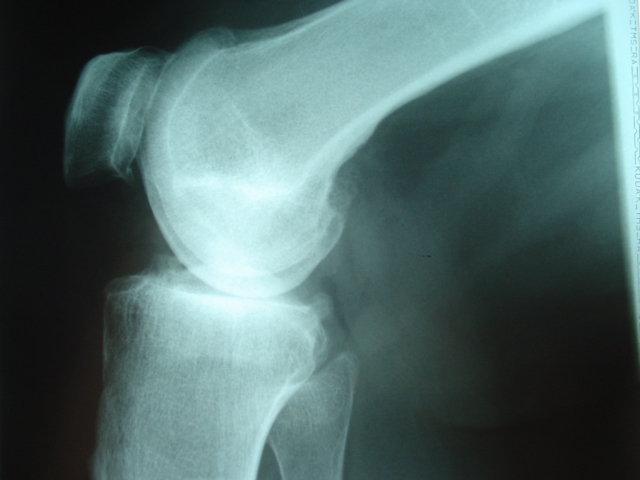
Figure 1B. Pre
op LAT xray of knee with Anteromedial Osteoarthritis
This
study however, compared two different pathologies i.e. Anteromedial Osteoarthritis and more extensive Osteoarthritis of
the knee. Past studies took advantage of the fact that at the
time of the study only one of the surgeons at Inverclyde Royal
Infirmary was undertaking hemiarthroplasty for Anteromedial
Osteoarthritis. The other two consultants concerned in the
study utilised a total knee replacement Kinemax in all patients
with Osteoarthritis of the knee.

Figure 2A. Post
op AP xray following Total Knee replacement.
Our
study was to determine if there was any difference in the
results of outcome in the different procedures for the same
pathology i.e. Anteromedial Osteoarthritis.Total Knee
replacement is an established and time proven procedure for both
Bicondylar and Unicondylar arthritis (10).

Figure 2B. Post op LAT xray following
Total Knee replacement
Our
results show that there is no significant difference in results
of both procedures for Anteromedial Osteoarthritis of the knee
in the short term. We plan to proceed with a long-term
review to establish any difference in the results.

Figure 3A. Pre
op AP xray Anteromedial Osteoarthritis.
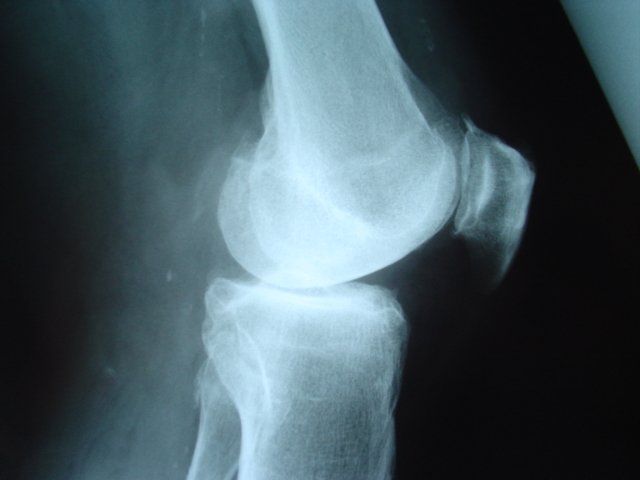
Figure 3B. Pre
op LAT xray Anteromedial Osteoarthritis.
Although this is a
retrospective study of relatively small numbers, it does focus
entirely on Anteromedial Osteoarthritis of the knee and the
short-term results clearly demonstrate that there is no
difference in the short-term results and therefore at this
moment in time justifies the continued use of a hemiarthroplasty
for Anteromedial Osteoarthritis of the knee.
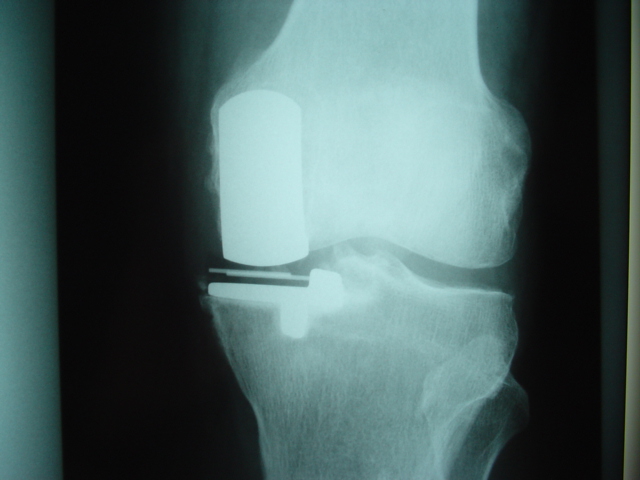
Figure 4A. Post op AP xray Oxford
knee replacement

Figure 4B. Post op LAT xray Oxford
knee replacement
References
1)
Perceptions of outcome after unicompartmental
and total knee replacement AE Weale,OA Halabi, Clinical
orthopaedics and related research, No 382,
pg143-153.
2) Oxford Medial unicompartmental
arthroplasty,A ten year survival study,
DW Murray,JW Goodfellow,JBJS 1998,80B,983-9.
3) Unicompartmental Vs Total knee
replacement in the same patient, Acomparitive study
CT Lairenin,SB Zelicof,RD Scot,Clinical
orthopaedics and related research,No 199,273;151-6
4) The mechanics of the knee and
prosthesis designs, J.W.Goodfellow,J.OConnor. Journal of Bone
and Joint surgery, 1978,No 3:60B358-369.
5) The wear of congruent meniscal
bearing in unicompartmental knee replacement. RW
Crawford,OConnor,JW Murray, Journal
of Bone and Joint surgery; 80-B;6;976-82;1998.
6) 10 years survival results of Oxford
mobile bearing uni knee arthroplasty in young patients.
A Price,U Svard ,DW Murray,JW Goodfellow ,I.S.TA
Chicago 1999
7.Osteoarthritis of the knee-A radiographic investigation.
Acta radiol (diagn)(stochl) suppl277,
1968:7-72.
8) Ahlbach.S,
The radiographic classification of medial
gonarthrosis. GW Keyes,AJ Carr,Acta
orthop scand,1992;63(5):497-501.
9) The swedish knee arthroplasty
register,A nation wide study of 30,003 knees 1976-1992. K
Knutson,S Lewold,L Lidgren,Acta Orthop scand1994:65(4)375-386.
10) Unicompartment or Total Knee
Replacement?Five year results of prospective randomised trial
of 102 osteoarthritic knees with unicompartmental arthritis J H
Newman,C.Ackroyd,N.Shah. Journal of Bone and Joint (B)
1998,80-b; 862-5
11) Oxford Medial Unicompartmental
arthroplasty.A survival analysis of an independent series Svard
U.G.C,Price A.J Journal of Bone and Joint(B) ;March
2001;83-B;191-4.
12) Swedish Knee Arthroplasty
Register1990-1998
13) 0xford Meniscal Bearing knee vs
Marmor knee in Medial Unicompartmental Arthroplasty S Lewold,S
Goodman,K Knutson,O Robertson,L LidgrenJournal of
Arthroplasty,10-6:722-31, 1995.
14) Does arthritis progress in the
retained compartments after Oxford Medial Unicompartmental
Arthroplasty. AE Weale,DW Murray,R Crawford,V Psychoyios,A
Bonomo,G Howell,J OConnor,JW Goodfellow
JBJS, 80B-5, 783-789,1999.
15)Anteromedial Osteoarthritis of the
knee S.H.White,P.F.Ludkowski,J.W.Goodfellow. Journal
of Bone and Joint surgery73B; 582,1991.
16) Questionnaire on the perceptions
of patients about Total Knee
Replacement.J.Dawson,R.Fitzpatrick,D.Murray,A,Carr. Journal of
Bone and Joint surgery, January1998;80-B;63-9.
|

