1.Bahuva Vishal D, M.S Ortho
2.Thakkar C J, M.S Ortho
3.Tawari Akhil A, M.S Ortho
4.Goregaonkar Arvind B, M.S Ortho , Prof and Head , LTMMC & LTMGH
Department and institution: Department Of Orthopaedics , LTMMC & LTMGHFrancisco, CA, USA
Address for Correspondence
Bahuva Vishal D, M.S Ortho
601, Matoshree apartments, Mithagar Road, Salviwadi,
Mulund (east), Mumbai-400 081
993046011
Email:vishesforu@gmail.com
|
|
Abstract: Femoroacetabular impingement is increasingly being considered as an important cause of idiopathic osteoarthritis of hip. We studied anteroposterior and lateral radiographs of 754 hips of Indian population to determine the prevalence of femoroacetabular impingement in india where unlike the west, primary osteoarthritis of the hip is rare. The prevalence of cam and pincer type of impingement was 4.9% which was statistically significant (p< .01%). The prevalence of isolated pincer type of impingement was 1%. The mean lateral centre edge angle was 38 degrees with a standard deviation of 3.8 degrees. The mean femoral head extrusion index was 0.31 with a standard deviation of 0.04. Femoral off-set of less than 10 mm was found in 4% of cases. A negative acetabular index was found in 5% of patients suggestive of pincer type of impingement. Os acetabuli were present in 3 % of the cases. Pistol-grip deformity present in 4% of cases. Alpha angle more than 55 degrees was noted in 4% of cases. The values though marginally less than western population still cannot explain such low incidence of primary osteoarthritis in Indian population. Further studies are still required to evaluate the nature of disease process, its natural history, actual cause and effect relationship between femoro-acetabular impingement and osteo-arthritis as well as better definition of its various parameters.
Key Points:
femoroacetabular impingement, prevalence, Indian population
J.Orthopaedics 2012;9(4)e9
Introduction:
Osteoarthritis of the hip is a debilitating and painful condition affecting a substantial proportion of the population. Idiopathic osteoarthritis accounts for approximately 40% to 50% of all cases of degenerative arthritis1 in western population and a growing body of literature supports the hypothesis that idiopathic osteoarthritis is frequently caused by subtle, and often radiographically occult, abnormalities at the femoral head-neck junction or acetabulum that result in abnormal contact between the femur and the acetabulum2.This condition, known as femoroacetabular impingement, has been proposed as the leading cause of labral tears, as well as degenerative hip arthritis.
Through observations at the time of open hip surgery, Ganz et al. defined the mechanisms of cartilage damage associated with femoroacetabular impingement as well as its clinical and radiographic features3,4. Although the association of femoro-acetabular impingement with hip osteoarthritis is well-known, little is known about the distribution of these malformations in a population-based setting or the magnitude of related clinical problems especially in India wherein primary hip osteoarthritis is rare. The main purpose of this study is to see whether femoroacetabular impingement is as significant a problem in Indian population as in western population.
methods:
We retrospectively evaluated the plain radiographs of 754 hips after obtaining the ethical clearance for the project. Patients belonging to age groups between 15 and 50 were included in the study. Patients with a past history of pain, fracture, surgery, dysplasia or osteonecrosis in the hip to be studied were excluded from the study. Measurements were made on the standard antero-posterior cross table lateral radiographs. Moses concentric circles were used to determine the centre of femoral head. Measurements were initially sub-classified into pincer type or the cam type.
Pincer type included the following
Lateral centre edge angle of Wiberg- It is formed by the intersection of a line drawn through the midpoint of the femoral head and a second line drawn from the centre of the femoral head to the upper outer margin of the acetabulum(figure 1) Acetabular index-The angle between the line joining the inner edge of acetabulum and the outer edge with the horizontal is the acetabular index
Acetabular Extrusion Index- the femoral head extrusion index, expresses the percentage of the femoral head diameter uncovered by the acetabulum, or the percentage of the femoral head lateral from perkin's line
Posterior Wall Sign-Posterior wall line should pass exactly through the centre of the femoral head
Os Acetabuli-Small accessory ossicles at the lateral margin of the acetabulum develop due to constant wear and tear. These accessory ossicles are known as os acetabuli(figure 2) .
Linear Indentation Sign-In pincer hips, corresponding linear indentation often occurs on femoral side with reactive cortical thickening
Cam type included the following parameters
Pistol Grip Deformity- Pistol grip deformity occurs due to the loss of concavity which is normally present at the antero-superior margin of the femoral head, on plain radiographs it looks like the rear end of the pistol (figure3)
Alpha Angle - Alpha angle is the angle between the femoral neck axis and a line connecting the head center with the point of beginning asphericity of the headneck contour ( figure 4).
Anterior Femoral Off-Set- It is defined as the difference in radius between the anterior femoral head and the anterior femoral neck on a cross-table axial view of the proximal femur.
Figure 1 – 23 years old female with centre edge angle of 50

Figure 2 – os acetabuli in a 41 years old male
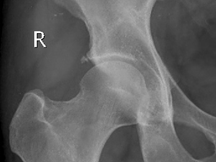
Figure 3- Pistol grip deformity in a 45 years old
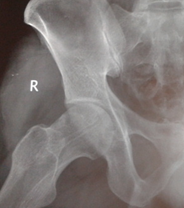
Figure 4- alpha angle more than 50 degrees

Results:
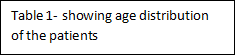
754 hips were included in the study with each hip evaluated using an antero-posterior and lateral radiographs. There were 211 males and 166 females.The age-wise distribution of patients is shown in table 1.
Age in years |
Percentage |
15-20 |
7 % |
20-25 |
12% |
25-30 |
19% |
30-35 |
17% |
35-40 |
20% |
40-45 |
11% |
45-50 |
14% |
The prevalence of cam and pincer type of impingement was 4.9% which was statistically significant (p< .01%). The prevalence of isolated pincer type of impingement was 1%. The mean lateral centre edge angle was 38 degrees with a standard deviation of 3.8 degrees. The mean femoral head extrusion index was 0.31 with a standard deviation of 0.04. Femoral off-set of less than 10 mm was found in 4% of cases. A negative acetabular index was found in 5% of patients suggestive of pincer type of impingement. Os acetabuli were present in 3 %of cases. Pistol-grip deformity present in 4% of cases. Alpha angle more than 55 degrees was noted in 4% of cases.
Discussion:
Femoroacetabular impingement (previously also called "acetabular rim syndrome") or "cervicoacetabular impingement" is a major cause of early osteoarthritis of the hip, especially in young and active patients. Though the concepts of impingement and the principles of treatment are nearly a century old, Ganz4 and his colleagues from Bern reintroduced these ideas in the 1990s in a series of papers reporting impingement in various conditions.
They have refined the concepts and proposed many patients with previously undiagnosed hip pain had more or less subtle deformities of the anterior femoral neck causing impingement and early osteoarthritis. It is characterized by an early pathologic contact during hip joint motion between skeletal prominences of the acetabulum and the femur that limits the physiologic hip range of motion, typically flexion and internal rotation. Depending on clinical and radiographic findings, two types of impingement are distinguished. Pincer impingement is the acetabular cause of femoroacetabular impingement and is characterized by focal or general overcoverage of the femoral head5. Cam impingement is the femoral cause of femoroacetabular impingement and is due to an aspherical portion of the femoral headneck junction6. Most patients (86%) have a combination of both forms of impingement, which is called "mixed pincer and cam impingement," with only a minority (14%) having the pure femoroacetabular impingement forms of either cam or pincer impingement7.
Though a number of parameters have been described the centre-edge angle of Wiberg is one of the most commonly used uniplanar discriminators of deep acetabular socket. Increasing age has been shown to influence the centre edge angle. In our study, since we included patients with age upto fifty years, we took a centre-edge angle of 45 degrees as the cut-off for pincer impingement. There is still some confusion in literature as to the exact limits of normal centre-edge angle. Some studies have taken 40 degrees as the cut-off limit of centre-edge angle whereas some others have taken 45 degrees. We have taken 45 degrees as the cut-off because there is a strong correlation between centre-edge angle of more than 45 degrees and significant hip pain due to labral tears. Thus there is still some obscurity as to the normal limits of centre-edge angle which need to be refined further. The angle between the line joining the inner edge of acetabulum and the outer edge with the horizontal is the acetabular5 index. It is positive in normal individuals. It becomes negative as acetabulum deepens.
The femoral head extrusion index, expresses the percentage of the femoral head diameter uncovered by the acetabulum, or the percentage of the femoral head lateral from Perkin's line. Cut-off value set at 25%. Any value less than 25% suggests pincer type of impingement. Posterior wall line should pass exactly through the centre of the femoral head. If it passes laterally, then it is suggestive of pincer type of impingement. If the line passes medially, then it is suggestive of cam type of impingement5.
Quantification of the amount of asphericity that is the cam type of impingement can be accomplished by the angle a, the femoral offset, or the offset ratio8. Angle a is the angle between the femoral neck axis and a line connecting the head center with the point of beginning asphericity of the headneck contour. An angle exceeding 50° is an indicator of an abnormally shaped femoral headneck contour. Another parameter for quantification of cam impingement is the anterior offset, which is defined as the difference in radius between the anterior femoral head and the anterior femoral neck on a cross-table axial view of the proximal femur. In asymptomatic hips, the anterior offset is 11.6 ± 0.7 mm; hips with cam impingement have a decreased anterior offset of 7.2 ± 0.7 mm9. As a general rule for clinical practice, an anterior offset less than 10 mm is a strong indicator for cam impingement.
We found the prevalence of femoro-acetabular impingement in our study to be 5%.The estimated prevalence, as described by Leunig M, Ganz R in Western countries is1015%.
Takeyama et al in 2009 found the incidence of femoro-acetabular impingement to be around 0.6% in Japanese population
. They believed that such a low incidence of femoro-acetabular impingement is consistent with a low incidence of primary hip osteo-arthritis in Japan. This discrepancy can be explained by the differences in the prevalence of osteoarthritis of hips in both countries. It is increasingly coming to notice that radiographs of idiopathic osteoarthritis of hip show signs of femoro-acetabular impingement. Indeed according to one study upto 71% of cases of idiopathic osteo-arthritis of hip show pistol-grip deformity. Therefore, there could be a causal association between femoro-acetabular impingement and idiopathic osteo-arthritis of hip and further studies are required for the same. One of the studies comprising of 85 hips in Indian population has found the prevalence of abnormal head-neck offset ratio at 11.7% and the mean alpha and beta angles of 45.6° and 40.6°, respectively. The authors concluded that the differences in the prevalence of hip osteoarthritis in Indian and western populations are not attributable to variation in the prevalence of abnormal head-neck offset but the authors also acknowledged small sample size included in their study10. Therefore, there could be a causal association between femoro-acetabular impingement and idiopathic osteo-arthritis of hip and further studies are required for the same.
Conclusion
Femoro-acetabular impingement is an increasingly recognized condition causing hip pain in young active adults and is believed to be a cause of hip osteo-arthritis. It describes a pathologic abutment between the femoral head and the acetabular rim. There are no large-scale studies to determine the magnitude of the disease problem in the general population in India. Our study is an observational study which shows a statistically significant 5% prevalence of femoro-acetabular impingement in India. There are very few available studies to compare the incidence with Western countries where the estimated prevalence is 8-15%. Further studies are still required to evaluate the nature of disease process, its natural history, actual cause and effect relationship between femoro-acetabular impingement and osteo-arthritis as well as better definition of its various parameters.
Reference:
Solomon L. Patterns of osteoarthritis of the hip. J Bone Joint Surg Br.
1976;58:176-83
Tanzer M, Noiseux N. Osseous abnormalities and early osteoarthritis: the role of hip impingement. Clin Orthop Relat Res. 2004;429:170-7.
Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005;87:1012-8
.
Ganz R, Parvizi J, Beck M, Leunig M, N¨otzli HP, Siebenrock KA.
Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112-20.
Tannast M , Siebenrock KA , Anderson SE . Femoracetabular impingement: radiographic diagnosiswhat the radiologist should know . AJR Am J Roentgenol 2007 ; 188 ( 6 ): 1540 1552
Jäger M, Wild A, Westhoff B, Krauspe R. Femoroacetabular impingement caused by a femoral osseous headneck bump deformity: clinical, radiological, and experimental results. J Orthop Sci 2004; 9:256 263
Ito K, Minka MA 2nd, Leunig S, Werlen S, Ganz R. Femoroacetabular
Impingement and the cam-effect. A MRI-based quantitative anatomical study of the femoral head-neck offset. J Bone Joint Surg Br. 2001;83:171-6
.
Nötzli HP, Wyss TF, Stöcklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral headneck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br 2002; 84:556 560
.
Tannast M, Zheng G, Anderegg C, et al. Tilt and rotation correction of acetabular version on pelvic radiographs. Clin Orthop Relat Res 2005; 438:182 190
Malhotra R, Kannan A, Kancherla R, Khatri D, Kumar V. Femoral head-neck offset in the Indian population: A CT based study. Indian J Orthop. 2012 Mar;46(2):212-5
|

