|
J.Orthopaedics 2007;4(4)e3
Introduction:
Cooper and Travers first described giant cell tumor of bone in
1818 (4). Bloodgood coined he term giant-cell tumor in 1912(1).
In 1940 Jaffe et al distinguished giant-cell tumor as a
distinct clinical, radiographic, and pathological entity that is
separate from other lesions containing giant cells(8). Giant
cell tumor of bone is characterized radiographically by a well
delineated, eccentric, purely lytic, epiphyseal lesion with the
absence of reactive sclerosis and periosteal new bone formation
abutting the articular surface. Giant cell tumor of the bone
accounts for 4-5% of primary bone tumors and 18.2% of benign
bone tumors. The incidence is increased in patients with Paget
disease of the bone, in which giant cell tumor is a rare
neoplastic complication. Typically, giant cell tumors occur in
skeletally mature patients aged 20-40 years. The incidence peaks
in those aged 20-30 years. Although intraosseous recurrence of
giant cell tumour is a well recognized complication; soft tissue
recurrences are rarely encountered
Case Report:
A
thirty-five year-old man was presented to our institution
because of a gradualy enlarging soft-tissue mass in the
anterolateral aspect of the proximal part of the right leg for
the past six monthsi. Twenty- four months previously, the
patient had been treated by curettage and packing with
polymethylmethacrylate cement for a giant-cell tumor of the
proximal aspect of the right tibia. Physical examination
revealed a nontender soft-tissue mass, seven by four centimeters
in size,mobile,variable in consistancy from bony hard to soft
cystic ; that was palpable in the anterolateral aspect of the
proximal part of the leg. Plain radiographs showed a
soft-tissue mass with more central ossification and
trabeculations (Figure 1-A). The curetted leison with
polymethylmethacrylate cement was intact. Magnetic resonance
imaging studies showed a lobulated well defined hyperintense
mass intending the proximal substance and origin of the
peroneus longus and peroneus brevis with loss of intervening fat
planes-possibly infiltrating the peroneus brevis on T2-weighted
and STIR images.Leison appeared iso to hyperintense to the
muscle on T1-weighted images.Hypointense areas suggestive of
mineralisd septae were seen within the leison.Hyperintense
cystic areas within the leison was also noted(Fig 1B).On
contrast study the leison showed heterogeneous enhancement(Fig
1C).The anterior and posterior intermuscular septum and the
interosseous membrane appeared normal.The patient was managed
with wide resection of the well circumscribed soft-tissue mass,
which measured 7 by 4.2 by 4 centimeters and was located in the
upper peroneal compartment attached to the peroneus brevis
muscle(Fig 1D). Histological analysis demonstrated a recurrent
giant-cell tumor(Fig 1E) .

Fig.1

Fig.2
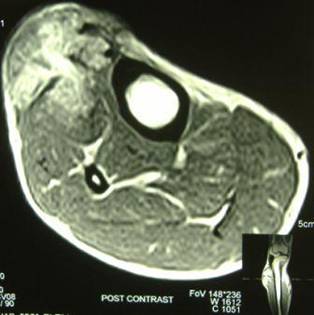
Fig.3

Fig.4
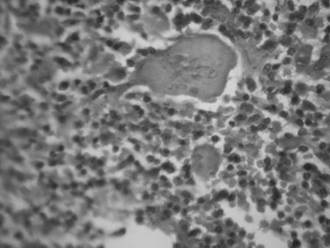
Fig.5
Discussion :
Intraosseous recurrences of giant cell tumor of bone are
common and readily recognized. ODonnell et al reported a 25%
rate of local recurrence with thorough curettage and packing
with polymethylmethacrylate (14). Radiologic evaluation of
recurrence typically reveals new areas of bone destruction at
the previous resection margin or resorption of intralesional
bone graft material (9,14,15,16,18,22,23).Recurrence of
giant-cell tumor after polymethylmethacrylate placement
typically reveals focal lobular destruction of bone about the
cement. Soft-tissue recurrences are less common. It is likely
related to either implantation at surgery or tumor spread
secondary to pathologic fracture. Soft-tissue recurrence may or
may not be visible on plain radiographs. Cooper et al. reported
seventeen cases of soft-tissue recurrence in their review of
1100 cases of giant-cell tumor (3). A peripheral rim of
ossification was noted around sixteen of the recurrent
soft-tissue tumors. In the one exception the ossification was
more centrally located within the soft-tissue mass. Other
studies (7, 19,21,) have also reported peripheral rim of
ossification around a soft-tissue recurrence of giant-cell tumor
including pulmonary metastasis, and this phenomenon is thought
to be almost pathognomonic of recurrence. Metaplasia of the
tumor cells may be responsible for this capability of pulmonary
and soft-tissue deposits to produce osteoid (3).The differential
diagnosis to be kept in mind is myositis ossificans. However
these recurrences can be differentiated from myositis ossificans
by their continued slow growth, their occurrence more than 2
months after surgery, and with time, the ossified mass should
increase, rather than decrease in size. The radiographic
appearance of the present reported case with more central
calcification without peripheral rim of ossification matches
that of the lone case reported in the series of Cooper et al.
Most giant cell tumours (80%90%) recur within
the first 3 years after initial treatment (6, 11, 12, 13, 17,
18, 22).After treatment, patients with GCT should be evaluated
with serial physical examinations and radiography of the
involved site and of the chest. Tumor recurrences have been
noted many years after initial treatment, and necessitate
long-term surveillance (10, 20). A local soft tissue tumor with
a peripheral rim of ossification in a patient with known giant
cell tumor of bone is essentially diagnostic of soft tissue
recurrence of giant cell tumor.
Reference :
with the Study of Bone Transplantation.
Ann. Surg., 56: 210-239, 1912.
2.2Campanacci, M.; Baldini, N.; Boriani,
S.; and Sudanese, A.: Giant-cell tumor of bone. J Bone and Joint
Surg., 69-A: 106-114, Jan. 1987.
3.Cooper KL, Beabout JW, Dahlin CD. Giant
cell tumor: ossification in soft tissue implants. Radiology1984;
153:597607.
4.Cooper AS, Travers B: Surgical Essays.
London, England: Cox Longman & Co; 1818: 178-9
5.Dahlin DC: Caldwell Lecture. Giant cell
tumor of bone: highlights of 407 cases. AJR Am J Roentgenol
1985 May; 144(5): 955-60
6.Dorfman HD, Czerniak B. Giant-cell
lesions. In:Dorfman HD, Czerniak B, eds. Bone tumors. St Louis,
Mo: Mosby, 1998; 559606.
7 . Ehara S, Nishida J, Abe M, Kawata Y,
Saitoh H,Kattapuram SV. Ossified soft tissue recurrence ofgiant
cell tumor of bone. Clin Imaging 1992; 16:
168-171
8 Jaffe, H. L.; Lichtenstein, Louis; and
Portis, R. B.: Giant CellTumor of Bone. Its Pathologic
Appearance, Grading, Supposed Variants and Treatment. Arch.
Pathol., 30: 993-1031, 1940
9 194. Kattapuram SV, Phillips WC,
Mankin HJ. Giantcell tumor of bone: radiographic changes
followinglocal excision and allograft replacement.
Radiology1986; 161:493498.
10 190. Kitano K, Shiraishi T, Iwasaki A,
Kawahara K,Shirakusa T. A lung metastasis from cell tumor ofbone
at eight years after primary resection. JpnJ Thorac Cardiovasc
Surg 1999; 47:617620.
11. Larsson SE, Lorentzon R, Boquist L.
Giant cell tumorof bone. J Bone Joint Surg [Am] 1975;
57:167173.
12. Manaster BJ, Doyle AJ. Giant cell
tumors of bone.Radiol Clin North Am 1993; 31:299323.
13. Mirra, J. M.: Giant cell tumors. In
Bone Tumors: Clinical, Radiologic, and Pathologic Correlations.
Vol. 2, pp. 941-1020. Philadelphia, Lea and Febiger, 1989
14.ODonnell RJ, Springfield DS, Motwani
HK, ReadyJE, Gebhardt MC, Mankin HJ. Recurrence of giantcell
tumors of the long bones after curettage andpacking with cement.
J Bone Joint Surg Am 1994;76:18271833.
15. Pettersson H, Rydholm A, Persson B.
Early radiologicdetection of local recurrence after curettageand
acrylic cementation of giant cell tumors. Eur JRadiol 1986; 6:1
4.
16. Remedios D, Saifuddin A, Pringle J.
Radiologicaland clinical recurrence of giant cell tumour of
boneafter the use of cement. J Bone Joint Surg Br 1997;79:2630.
17 Resnick D, Kyriakos M, Greenway GD.
Tumorsand tumor-like lesions of bone: imaging and pathology of
specific lesions. In: Diagnosis of bone and joint disorders. 3rd
ed. Philadelphia, Pa: Saunders,1995; 36283938.
18 Richardson ML, Lough LR, Shuman WP,
Lazerte GD, Conrad EU. MR appearance of skeletal neoplasms
following cryotherapy. Skeletal Radiol 1994;23:121125.
19 . Serra, J. M.; Muirragui, A.; and
Tadjalli, H.: Extensive distal subcutaneous metastases of a
"benign" giant cell tumor of the radius. Plast. and Reconstr.
Surg., 75: 263-267, 1985.
20 . Scully SP, Mott MP, Temple HT, OKeefe
RJ,ODonnell RJ, Mankin HJ. Late recurrence of giantcelltumor of
bone: a report of four cases. J BoneJoint Surg Am 1994;
76:12311233.
21 Tubbs, W. S.; Brown, L. R.; Beabout, J.
W.; Rock, M. G.; and Unni, K. K.: Benign giant-cell tumor of
bone with pulmonary metastases: clinical findings and radiologic
appearance of metastases in 13 cases. AJR: Am. J. Roentgenol.,
158: 331-334, 1992
22 . Unni KK. Dahlins bone tumors:
general aspectsand data on 11,087 cases. 5th ed. Philadelphia,
Pa:Lippincott-Raven, 1996
23 Waldman BJ, Zerhouni EA, Frassica FJ.
Recurrenceof giant cell tumor of bone: the role of MRI in
diagnosis.Orthopedics 1997; 20:6769.
|

